The back pain is unrelenting. The x-ray shows some curvature of the spine. What is Scoliosis? What causes Scoliosis? Can the curve progress? Do patients with Scoliosis have more back pain? What are the non-surgical treatment options for Adult Degenerative Scoliosis? Let’s dig in.
Collaboration is key for the best clinical results. The Centeno-Schultz Clinic works with the very best physical therapists and chiropractors. Dr. Chris Gubbels is a trusted chiropractor in Fort Collins who has advanced certification in Chiropractic Biophysics and specializes in the treatment of scoliosis. He has provided excellent care for some of our patients in northern Colorado with tremendous results. Dr. Gubbels is the author of this blog.
Non-Surgical Treatment Options for Adult Degenerative Scoliosis
Scoliosis is a major health problem affecting people ranging in age from infants to geriatrics. There are different types and causes of scoliosis. 80% of scoliosis affecting children is idiopathic scoliosis. Idiopathic means there is no known exact cause, however, there are likely both genetic and environmental influences. Adult scoliosis may be scoliosis present as an adolescent that is still presenting in adulthood or it may be new scoliosis that developed in adulthood.
What Is Scoliosis?
Scoliosis is diagnosed when there is 10° or more lateral bending in the spine with rotation present. Scoliosis is actually a three-dimensional spine deformity, meaning the disc and vertebrae actually grow asymmetrical.
What Causes Scoliosis?
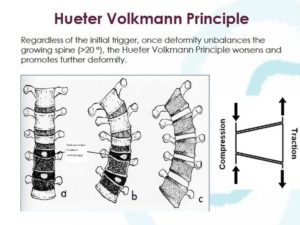
Although the exact cause is unknown in idiopathic scoliosis the progression is well understood once it begins. As the spine begins to lateral bend and rotate, the inside of the curve is compressed while the outside of the curve is pulled or under traction. In a growing spine, the compression on the inside of the curve decreases the growth, while the traction on the outside of the curve increases growth causing the vertebrae to continue to grow asymmetrically which can cause scoliosis curve to progress. This is known as the Hueter Volkmann Principle. Other less common causes of scoliosis are neuromuscular discord such as Arnold Chiari malformation, a congenital misshaped vertebrae, neurofibromatosis, connective tissue disorders such as Marfan’s or Eheler-Danlos, trauma-induced and post-surgical scoliosis.
Scoliosis in Adults
Scoliosis in an adult can either be the continuation of scoliosis that started in adolescence or new scoliosis that develops in adulthood known has degenerative de novo scoliosis. This adult de novo scoliosis can occur due to disc and spinal joint degeneration, pelvic obliquity secondary to hip pathologies or leg length inequalities and/or metabolic bone disease. Degenerative scoliosis affects 38% of adults between the ages of 40-90yo, with a greater prevalence in women and in adults impacted past the age of 60.[1] Changes in the structure, function and physiological alignment of the spine lead to asymmetrical loading which provokes further degenerative changes, accelerated curve progression, muscle changes and postural collapse. Factors that impact the risk of curve progression include: Size of curve, location of curve, amount of rotation or twisting of the spine, side-to-side misalignment of the bones of the spine, and the position of the lowest vertebrae in the low back in relation to the height of the pelvis.
Risk of Curve Progression
In adolescents, curves have their greatest risk of progression during growth spurts. The highest risk of curve progressing is during the first 1-2 years of puberty when adolescents grow the fastest, which is known as peak height velocity. Because of this, the Scoliosis Research Society recommends that girls are screened twice for scoliosis at the ages of 10 and 12, and boys are screened for scoliosis between the ages of 13-14. Early screening leads to earlier detection, earlier interventions, and better outcomes.
In adults, adolescent curves can continue to progress. Generally speaking adolescent curves in adulthood >30° have a moderate risk of progression and curves over >50° have a very high risk of progression. There are many other factors that can increase the risk of scoliosis curve progressing in adulthood including having an anatomical short leg, a large amount of rotation in comparison to the amount of lateral bending, segmental instability demonstrated by lateralisthesis, and metabolic disease to name a few. Additionally, curves located in the lumbar spine and thoracolumbar spine have a higher risk of progression than thoracic scoliosis in adults.
Do Adults with Scoliosis Have More Back Pain?
Adolescents with scoliosis frequently have low-grade spine pain. Some research suggests that greater curve severity is correlated with increase pain levels in adolescents[2]. Adults with scoliosis have more than double the rates of back pain compared to non-scoliotic adults. Scoliotic deformities in the lumbar spine correlate with a loss of the normal lumbar lordosis, directly impacting low back pain[3]. Adults with scoliosis demonstrate greater functional limitations, greater daily analgesic use report worse health-related quality of life (HRQoL) compared to adults without scoliosis. Frequent symptoms in adults with progressive scoliosis included both back pain, vascular issues in the legs and neurological symptoms, similar to sciatica
Treatment Options
Reduction in pain and improvement in the quality of life are the primary goals of both surgical and non-surgical treatment options for scoliosis. Surgical interventions should be reserved for cases when all conservative methods of treatment have failed.
Low profile custom Scolibrace in an adult with progressive, painful degenerative scoliosis
Treatment options including chiropractic adjustments, general physical therapy, yoga, and massage therapy have not been found effective in slowing scoliosis curve progression or improving curve (curvature?) but may provide temporary pain relief and improve spine function and mobility.
In adolescents, scoliosis-specific exercises such as SEAS (Scientific Exercises Approach to Scoliosis), Schroth and Chiropractic BioPhysics, and soft bracing can be effective in treating smaller curve (curvatures?), generally under 20°. In curves greater than 20° in growing adolescents, scoliosis-specific exercises or an intensive scoliosis-specific rehabilitation program combined with custom rigid bracing is the most effective treatment option.
Scoliosis-specific exercises and custom scoliosis bracing have been found effective in both reducing back pain and slowing and possibly stopping curve progression in adults.[4-6] Palazzo et al. found that adult degenerative curves progressed 1.5° per year with observation only (no treatment). Curve progression was reduced to .2° with wearing a scoliosis brace 4-6 hours daily.[7] Scoliosis exercises or bracing alone can decrease pain and/or improve posture, but the best results are achieved when using wearing a brace combined with scoliosis exercises. Additional research has demonstrated that scoliosis treatments, including custom bracing, that work to restore lumbar lordosis in scoliotic patients are effective in reducing low back pain[3]. SOSORT (International Society on Scoliosis Orthopedic and Rehabilitation Treatment) recommends both scoliosis-specific rehabilitation programs and bracing for adults with progressive scoliosis and back pain for patients that are not good surgical candidates or to try non-surgical treatment options before perusing surgery.
Not All Treatments Are The Same
While general physical therapy and chiropractic have not been found effective in slowing the progression of scoliosis or improving the scoliosis curve, there are chiropractors and physical therapists trained in scoliosis-specific techniques that have been found effective in treating scoliosis. Specifically, both chiropractors and physical therapists may have specialized training in SEAS (Scientific Exercise Approach to Scoliosis) and/or Schroth, which are scoliosis-specific exercise approaches to treating scoliosis. Chiropractic BioPhysics (CBP) is an advanced chiropractic technique that combines specific exercises and traction to correct spine deformities. CBP has published over 240 research papers on its effectiveness in treating scoliosis, and in correcting cervical, thoracic and lumbar curves when viewed from the side.
Additionally, not all braces are the same, in fact, bad braces get bad results. Many braces work to try to hold the spine in its deformity in hopes the curves will not progress. Scolicare is a true three-dimensional bracing system that works by putting the spine in a corrected position that helps the spine grow more correctly in adolescents and may improve some curves and spinal alignment and balance in adults. With Scolicare each brace is custom made with computer-aided design and manufacturing to make a custom brace for every patient.
About the Author:
Dr Chris Gubbels is a Fort Collins Chiropractor, with advanced certification in Chiropractic BioPhysics, located at Square ONE Advanced Spine Correction. Dr. Gubbels specializes in non-surgical spine correction and rehabilitation with a specialization in spine deformities and scoliosis bracing. He is an active member of SOSORT and is Colorado’s leading Scolibrace provider. Through their trained providers, Scolibrace makes custom scoliosis and kyphosis braces for infants, adolescents, and adults. To learn more about non-surgical treatment options visit www.squareonehealth.com.
Monticone, M., et al., Adults with idiopathic scoliosis improve disability after motor and cognitive rehabilitation: results of a randomised controlled trial. Eur Spine J, 2016. 25(10): p. 3120-3129.
Park, J.H., H.S. Jeon, and H.W. Park, Effects of the Schroth exercise on idiopathic scoliosis: a meta-analysis. Eur J Phys Rehabil Med, 2018. 54(3): p. 440-449.
Palazzo, C., et al., Effects of Bracing in Adult With Scoliosis: A Retrospective Study. Arch Phys Med Rehabil, 2017. 98(1): p. 187-190.
Download Your free copy of Dr. Centeno’s groundbreaking work on spinal health and how Interventional Orthopedics can help you avoid life-altering surgery.