The headaches and dizziness have been debilitating. Your doctor suspects that you have an injury to the upper cervical ligaments. What are the Alar ligaments? What is the Alar Ligament Test? Are there other Alar Ligament tests? Let’s dig in.
What Are the Alar Ligaments?
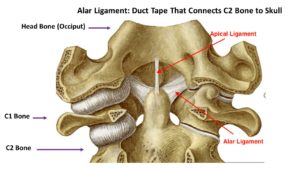
Ligaments are thick bands of connective tissue that connect one bone to another. The Alar ligament connects the upper neck to your head. A brief review of anatomy and terminology is helpful. The cervical spine has 7 building blocks which are numbered C1-7. These building blocks are called vertebral bodies. The top vertebral body referred to as C1 meets with the base of the skull which is called the occiput. The C1 vertebral body stacks upon the C2 vertebral body. The C2 vertebral body has a unique boney prominence that resembles the Washington monument. It is called the Odontoid Process or Dens. The Alar ligament connects the boney prominence of C2 with the occiput. There is a right and left Alar ligament. In summary, the alar ligament is a critical ligament that connects your neck to your head.
What Is the Alar Ligament Test?

There are different Alar ligament tests that are used. The most common are those used during a physical examination by either your doctor or physical therapist and those used during a specialized radiographic study.
Physical Examination Tests

Lateral Flexion: While seated the boney prominence of C2 is identified and slight compression on the crown of the head is applied. The patient is then placed into the right and left side bend. This involves directing the patient’s ear towards their shoulder on the same side A positive test is when there is a lag in the movement or side to side difference (1). Please see Figure A.
Rotation Stress Test: Needs to be performed in flexion, extension, and neutral. The C2 is stabilized with one hand while the top of the head is gripped with the other hand (2). The head is then rotated both to the right and the left. Excessive movement is consistent with an Alar ligament injury. Illustrated in Figure B.

Lateral Shear Test: The patient is seated with pressure applied to the boney prominence of C1 ( transverse ligament). Pressure is then applied from one side of C1 causing a shearing force between the C1 and C2. If there is movement the test is positive. Figure C
The accuracy and predictability of the tests are dependent upon many factors one of which is the experience of the practitioner who is performing the examination. When all three tests are used together, they are more accurate and predictive of an alar ligament injury (3). Unfortunately, all manual examinations and their findings have limitations. It is for this reason that the gold standard of determining an alar ligament injury is MRI (4).
Are There Other Alar Ligament Tests?
Yes! The radiographic imaging that your doctor or orthopedic surgeon orders, unfortunately, does not extend up to the C1/2 level but rather stops at C2. Therefore traditional imaging is not helpful as it does not evaluate the Alar ligaments and their integrity. Fortunately, there are specific radiographic studies that can be used to evaluate the Alar ligaments. Special radiographic tests are required to evaluate the Alar ligaments. These are not static studies like traditional MRI’s and x-rays. Rather they involve movement which is essential to determine the presence of instability. The most common radiographic Alar ligament tests are:
Digital Motion X-Ray
Digital motion x-ray also called DMX is a recorded x-ray of the upper cervical spine while the patient moves (5). The patient is put through different movements that include flexion forward, extension, and lateral side bending. Specific measurements are taken which are used to determine the integrity of the alar ligament. The most common measurement is the amount of overhang of the C1 on C2, The is the amount of motion that occurs between the C1 and C2 bone when the patient side bends their head (6). Dr. Katz of Katz Chiropractic in Boulder Colorado is an expert in DMX and chiropractic management of upper cervical injuries shared a recent abnormal DMX that is shown below. The white cursor identifies the multiple injuries.
Upright MRI
Traditional MRI involves the patient lying on their back in a tube. Unfortunately, this does not mimic the forces of daily life which include gravity. A specialized MRI has addressed this issue and has patients sitting upright. Upright MRI also allows patients to be put through different maneuvers similar to daily living. The movements include flexion, extension, and lateral side bending. Upright MRI is very useful in the diagnosis of Alar ligament injuries. To learn more about Craniocervical instability and use of an upright MRI as an Alar ligament test please watch the video below.
In Conclusion
The Alar ligament is a thick band of connective tissue that connects that C2 vertebral body to the skull. Alar ligament tests involve those used during a manual physical examination and specialized radiographic tests. The lateral flexion, rotation stress test, and lateral shear test are three specific manual Alar ligament tests. They are best used together as opposed to separately. Manual examinations have limitations and therefore the gold standard for evaluating alar ligament injuries is a specialized MRI. Traditional imaging is not a useful Alar ligament test. Rather specialized tests are required which include Digital Motion x-ray and Upright MRI. The Centeno-Schultz Clinic are experts in the evaluation and management of upper cervical ligament injuries. We have pioneered the first nonsurgical treatment for Craniocervial instability using a patient’s own bone marrow-derived stem cells.
If traditional imaging and medical care have failed to determine why your headache, dizziness, and brain fog persist please schedule a telemedicine consultation with a board-certified, fellowship-trained physician who can review your history, current imaging, and determine your injury and appropriate nonsurgical treatment options. Stop the suffering and contact us today.
Could Craniocervical Instability Be the Cause of Your Symptoms?
Imaging-Get movement based imaging (DMX or Upright MRI with flexion and extension).

Get Typed via a Telemed Appointment-There are 8 different types of CCI based on which ligaments are Injured.

Exam-If you’re a candidate for precise orthobiologic injections, you fly in for an exam and treatment. A hands-on exam refines what we need to treat.
Treatment-Get treated with a CCI focused, orthobiologic treatment plan tailored to you. That includes PICL or whichever image guided, precise injections are the most likely to help you.
1.Osmotherly PG, Rivett DA, Rowe LJ. Construct validity of clinical tests for alar ligament integrity: an evaluation using magnetic resonance imaging. Phys Ther. 2012 May;92(5):718-25.
2.Peter Grant Osmotherly, Darren Rivett, Lindsay J. Rowe, Toward Understanding Normal Craniocervical Rotation Occurring During the Rotation Stress Test for the Alar Ligaments, Physical Therapy, Volume 93, Issue 7, 1 July 2013, Pages 986–992, https://doi.org/10.2522/ptj.20120266
3.Kaale BR, Krakenes J, Albrektsen G, Wester K. Clinical assessment techniques for detecting ligament and membrane injuries in the upper cervical spine region–a comparison with MRI results. Man Ther. 2008;13(5):397-403. doi:10.1016/j.math.2007.03.007
4.Harry Von P, Maloul R, Hoffmann M, Hall T, Ruch MM, Ballenberger N. Diagnostic accuracy and validity of three manual examination tests to identify alar ligament lesions: results of a blinded case-control study. J Man Manip Ther. 2019;27(2):83-91. doi:10.1080/10669817.2018.1539434
5.Freeman MD, Katz EA, Rosa SL, Gatterman BG, Strömmer EMF, Leith WM. Diagnostic Accuracy of Videofluoroscopy for Symptomatic Cervical Spine Injury Following Whiplash Trauma. Int J Environ Res Public Health. 2020;17(5):1693. Published 2020 Mar 5. doi:10.3390/ijerph17051693
6. Radcliff KE et al. Does C1 fracture displacement correlate with transverse ligament integrity? Orthop Surg 2013;5(2):94-9. https://www.ncbi.nlm.nih.gov/pubmed/23658043