Shoulder Joint Pain: What You Need To Know
Get Help With Shoulder Joint PainShoulder joint pain is the third most common reason that people see their primary care physician (1). It is commonly experienced by people who use their hands overhead a lot, particularly in occupations such as painting and construction.
Individuals who train with repetitive overhead movements, such as tennis players, swimmers, and basketball players, are also prone to develop shoulder joint pain.
The symptoms and progression of pain in the shoulder joint can vary from person to person, depending on what is causing it. We’ll discuss the causes of shoulder pain, how it is diagnosed, and how it is treated.
Getting To Know The Shoulder Joint
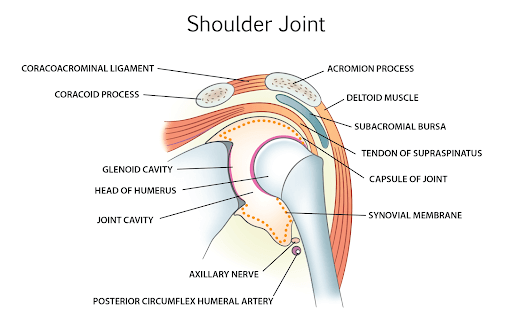
The shoulder is composed of two major joints: the large glenohumeral (GH) joint and the smaller acromioclavicular (AC) joint.
The GH joint is a ball and socket joint. The head of the humerus (the arm bone) fits snugly into a boney socket called the glenoid. The surfaces of both bone are covered with articular cartilage which allows the bones to smoothly slide across one another. The joint has a capsule which is a cellophane-type wrapping across the joint. The capsule provides stability, support, and protection of the joint.
The AC joint is smaller and is the union of the collar bone (clavicle) and the acromion. Like the GH joint, the AC is lined with cartilage and enveloped by a connective tissue capsule.
Joint Surface
A synovial membrane lines the inner surface of the capsule. It releases synovial fluid which reduces friction between the joint surfaces. Think of the synovial fluid as the WD 50 for the joint.
Glenoid Labrum
The socket of the GH joint is called the glenoid. It is a shallow cup that enables the joint to perform some amazing ranges of motion: flexion, extension, abduction, adduction, internal, and external rotation. The glenoid labrum is a small fibrocartilage cup seated within the glenoid that provides joint stability and aids against dislocation. The labrum continues with the biceps brachii tendon.
The humeral head is much larger than the boney cup (glenoid), which allows for a wide range of motion. However, for the same reason, it is also one of the most commonly dislocated joints. The glenoid labrum helps to stabilize the joint and reduces the risk of this occurring.
Muscles
The muscles also help to stabilize the joint.
The shoulder muscles that form a part of the joint and connect it to the humerus, clavicle, and scapula and include the deltoid, teres major, supraspinatus, infraspinatus, teres minor, subscapularis, trapezius, latissimus dorsi, levator scapulae, rhomboid major, rhomboid minor, serratus anterior, pectoralis major, pectoralis minor, subclavius, coracobrachialis, biceps brachii, and triceps brachii.
The rotator cuff is a group of four muscles and their tendons.. They provide stability and movement in the shoulder joint. The four muscles are:
- Supraspinatus
- Infraspinatus
- Teres Minor
- Subscapularis.
Bursae
A bursae is a small fluid-filled sac that is locaed at various boney locations within the body. They are situated between bone and tendon, muscles and ligaments. They reduce the friction and allow tendons, muscles, and ligaments to glide smoothly over boney surfaces.
There are also multiple synovial bursae within the shoulder acting as cushions between the tendons of these muscles in the shoulder. These include the subacromial, subscapular, subcoracoid bursa, and subscapular bursa. The bursae reduce friction between joint surfaces.
Ligaments
Ligaments are thick pieces of connective tissue that connect bone to bone. There are an extensive number of ligaments within the shoulder that include: superior, middle, and inferior glenohumeral ligaments, coracohumeral, coracoacromial, AC joint, and coracoclavicular ligaments. These ligaments function collectively to provide stability for the shoulder joint.
The shoulder ligaments provide critical support and stability for the shoulder. The ligaments that support the joint include the glenohumeral ligaments, coracoclavicular ligaments, and coracohumeral ligaments. Ligaments stabilize the joint and hold the bones across the joint in place together.
Blood Supply
The axillary artery supplies blood to the shoulder. Its branches include the superior thoracic artery, thoracoacromial artery, lateral thoracic artery, subscapular artery, anterior humeral circumflex artery, and posterior humeral circumflex artery. These arteries supply blood not just to the shoulder but to the entire arm as well.
Nerve Supply
The nerves supplying the shoulder joint are the suprascapular, lateral pectoral, and axillary nerves. All of the nerves originate from the brachial plexus. This is a network of nerves that are made of the lower cervical nerves and the thoracic nerve (C5, C6, C7, C8, and T1).
The Symptoms Of Shoulder Joint Pain
The symptoms of shoulder joint pain vary, depending on the cause, location, and severity of the underlying issue.
The most common symptoms include:
Pain: It can be mild, moderate or severe. Onset can be gradual or abrupt. It may be constant or intermittent. The pain can be localized in different areas: front, back, side, or top of the shoulder. The pain may also radiate down a portion of the arm.
Restriction in Range of Motion: Shoulder joint pain is often associated with limited range of motion. Patients often complain of difficulty with raising, extending, and flexing their shoulder joint. Audible crackling and popping may also be present and is referred to as crepitus. In severe cases patients are unable to raise their arms overhead to dress or lift a heavy object.
Swelling and Redness: In some cases, the shoulder joint may become swollen with areas of redness in the skin. Commonly, shoulder joint pain can be dull, aching, sharp, or even radiate down to the rest of the arm and forearm. There may also be redness and swelling of the joint. In some cases, the joint may be warm and have crepitus or air under the skin.
Along with pain, range of motion of the joint is often affected. This includes abduction, adduction, flexion, extension, external rotation, internal rotation, horizontal adduction (transverse flexion), and horizontal abduction (transverse extension).
So a person would not be able to raise their arms overhead to dress or lift a heavy object. Overall movement of the upper arm is affected. This can begin to affect quality of life.
Causes Of Shoulder Joint Pain
The shoulder is a complex joint with multiple structures that include bone, muscles, tendons, ligaments, nerves, labrum, and blood vessels that are susceptible to injury and degeneration. Injury to any of the structures can lead to shoulder joint pain.
An expert in interventional orthopedics/biologics can identify the cause of your pain and non-operative treatment options. The most common causes of shoulder joint pain are:
Bursitis
A bursae is a fluid-filled sac that allows tendons, muscles, and ligament to smoothly slide across boney areas in the body.
Inflammation of the bursae within the shoulder joint can cause shoulder pain. Of all the bursa in the shoulder joint, the most commonly affected bursa is the subacromial bursa. This bursa is present below the acromion process of the shoulder and is most affected since it acts as a cushion for repeated overhead movement.
Tendinitis
Tendons are thick pieces of connective tissue that connect muscle to bone. Tendons play an important role in shoulder movement. Tendonitis is a medical condition characterized by inflammation or irritation of a tendon.
It commonly occurs as a result of overuse, repetitive movements, poor throwing mechanics, or trauma. It can also occur from infection. Common symptoms include pain, swelling, stiffness, weakness, and restriction in range of motion.
Tendinitis can occur in any tendon but is common in the rotator cuff. The rotator cuff is composed of four muscles and their tendons. They include the supraspinatus, infraspinatus, subscapularis, and teres minor. Rotator cuff tendinitis is a common cause of shoulder pain.
Tendon Tears
Tendons are thick pieces of connective tissue that connect muscle to bone. They are susceptible to injury. There are four types of tendon tears.
- Grade 1: stretch injury with all fibers intact
- Grade 2: partial thickness tear
- Grade 3: full thickness tear
- Grade 4: full thickness tear with retraction, where the tendon is separated into two parts
A tear in the tendon can result in significant shoulder pain. As the rotator cuff muscles have an integral role in the shoulder, rotator cuff tendons are susceptible to injury. This can result from trauma or overuse, particularly in the dominant shoulder.
Risk factors for shoulder injuries including smoking, hypercholesterolemia, poor posture, certain sports, and occupational tasks. A class of antibiotics called fluoroquinolone has been associated with tendinopathy and tendon rupture (4).
The most common fluoroquinolone currently prescribed is ciprofloxacin. People with tendon tears often experience night pain often along with restriction in range of motion. Tendon tears can be a partial thickness or full thickness tear.
Impingement
Shoulder pain can be a chronic relapsing symptom of shoulder impingement where the tendon or the bursae can get impinged under the acromion process during overhead movements. There are two types of shoulder impingement: external and internal impingement syndrome.
External impingement is the more common type of shoulder impingement and involves compression of the tendons and the subacromial bursae between the head of the humerus and the acromion. It is mostly due to inflammation, irritation, and degradation of the parts of the joint within the subacromial space.
Internal impingement is due to the repetitive impingement caused by overhead work by throwers and manual laborers. The compression occurs between the rotator cuff tendons and the shoulder socket (glenoid) and labrum.
Shoulder Instability
Anterior shoulder instability, also known as glenohumeral instability, occurs when the shoulder has abnormal laxity, whether from traumatic and non-traumatic injury to the shoulder ligaments, labrum or muscles.
As a result, the humerus can shift or move partially (subluxation) or completely (dislocation) out of the socket.
Shoulder instability could be uni- or multi-directional. It can occur congenitally, or due to repeated microtrauma, major trauma, a recurrence, or a combination of all of the above.
Arthritis
Arthritis of the shoulder joint can cause chronic shoulder pain, where the articular surface of the humeral head and glenoid are gradually degraded due to inflammatory cells and markers. Arthritis can also occur in the AC joint leading to restriction in range of motion and shoulder pain on the top of the joint.
Types of arthritis include inflammatory arthritis, rheumatoid arthritis, osteoarthritis, or infectious arthritis. t Arthritis can lead to pain and loss of function of the shoulder joint.
Labral Tear
The shoulder labrum is a ring of fibrocartilage situated on the socket bone(glenoid). It deepens the shoulder socket, increasing the surface area and provides attachments for shoulder ligaments and tendons. It is important to the stability and function of the shoulder. It is susceptible to injury and degeneration.
The glenoid labrum, the ring of cartilage around the shoulder joint, can tear when injured (either from acute trauma or gradually over time). There are two common labral tears: a Bankart lesion and a superior labral tear from anterior to posterior (SLAP tear).
Labral tears can increase the risk of shoulder dislocation and cause a dull throbbing pain and difficulty sleeping due to shoulder discomfort.
Frozen Shoulder
A frozen shoulder, also known as adhesive capsulitis, is a painful condition that gradually progresses over many months. It is an inflammatory condition where the GH joint capsule gradually undergoes thickening and fibrosis.
Clinically there is progressive stiffness and limitation of range of motion, particularly external rotation. The recovery is slow and can take about 2 years. Although the etiology is not known, it is more common in women and in the non-dominant shoulder.
Shoulder Dislocation
Shoulder dislocations represent nearly half of all the dislocations that occur in the human body. The shoulder can dislocate anteriorly, posteriorly, or in a downward direction. The anterior dislocation is the most common. It can be a complete dislocation or a partial dislocation. The fibrous tissue that joins the bones can tear due to huge force or extreme rotation.
Contact sports, trauma from motor vehicle accidents, and falls can “pop” the joint out of its shallow socket. leading to shoulder pain.
People who have had a previous dislocation are more likely to have a subsequent dislocation in the future due to the laxity of the tissue. A higher incidence of dislocation is also seen in individuals who have torn rotator cuffs or glenoid fractures.
Dislocations require medical attention as recurrent dislocations put the shoulder at risk for additional injuries. Examples include post-traumatic arthritis, injury to the labrum, bone, and rotator cuff.
Regenerative injections with PRP or bone marrow concentrate can be effective in increasing blood flow and healing to the loose or injured shoulder capsule and ligaments.
Fractures
Fractures in the shoulder joint are mostly due to proximal humeral fractures. These can occur due to falls and trauma.
Fractures are often accompanied by damage to the blood vessels and the nerves in the shoulder as in any crush injury where the accompanying nerves and vessels running along the bone are injured. These injuries often cause sharp and severe shoulder pain along with loss of function of the shoulder joint which require emergent medical attention.
Bone Spurs
A bone spur, also known as an osteophyte, is typically found at the edge of a bone at a joint. Bone spurs are typically the result of instability, friction, and stress. It is the body’s attempt to create stability.
Due to repeated wear and tear from continuous friction, osteophytes (or small bony protrusions) start growing and can calcify, leading to acromion and subacromial spurs.
Bone spurs are often associated with rotator cuff tears. Although the relationship is not well understood, the association between bone spurs and rotator cuff injury is well documented. Studies show that heel-type spurs are a risk factor for full-thickness rotator cuff tears (2).
Initial Management Of Shoulder Pain At Home
There are many ways to manage your shoulder pain at home. These supportive treatments should relieve your pain completely in the first few weeks. Here are some common ways to manage shoulder pain at home:
- Be Conscious Of Your Posture
Maintain good posture throughout the day when sitting, standing, and sleeping. Good posture supports the muscles spread across the shoulder bone and the joint. An improper posture pulls the muscles unevenly across the back placing strain and pressure on both the muscles and associated tendons. If left uncorrected, this can lead to injury of the rotator cuff, and the opposite shoulder joint is strained.
Change positions frequency so that you don’t strain one group of muscles. Use an ergonomic chair so that your spine is supported when working at a desk. - Rest As Needed
Make sure to incorporate plenty of rest throughout the day to avoid overloading the injured area. Modify painful activities, such as using a trolley while shopping instead of a basket. Don’t overreach for things overhead, and instead ask someone to help you. Avoid repetitive movements that can worsen shoulder pain, such as vacuuming and ironing. - Exercise Lightly
Avoid repetitive overhead movements that can worsen shoulder pain so exercise with simple movements. No jumping rope or sports like tennis or basketball. Gentle flexion and extension not beyond the angle where pain results. Stop when there’s pain. No need to work out through the pain. - Make Use Of Pain Relievers
Over-the-counter (OTC) painkillers can provide pain relief when used appropriately. Alternating between heat and ice therapy can help to reduce pain, depending on the cause of the symptoms.
Managing Shoulder Pain At Work
Shoulder pain can be extremely uncomfortable, and begin to affect concentration and productivity. So, how do you go about working when you have pain in the shoulder joint? Here are some steps you can take:
- If you have a desk job, make sure to set up your desk properly with an ergonomic chair and the computer monitor set at eye level
- For those who have to use the telephone, use headphones or a headset so that you don’t have to twist your neck to support the handset
- Incorporate gentle movement or stretches throughout the day, such as rolling your shoulders
- If you work at a job that requires overhead lifting, consider changing the lifting technique or use hand trucks, pushcarts, or a forklift for heavier loads
- Consider taking a hot bath with magnesium sulfate, which can soak through the skin and relax tight muscles
When To See A Doctor
While shoulder joint pain can resolve on its own within a few weeks, certain signs and symptoms should prompt you to see a doctor immediately. Here’s a list of symptoms to watch out for along with pain in the shoulder joint:
- Any unexplained masses, swelling, or deformity in the shoulder area, especially if you have had a history of a benign or malignant tumor
- Redness of the skin or fever as these are signs of infection and may need treatment with antibiotics
- If the injury was caused by trauma, such as a fall or accident, as this could result in a dislocation, tear, or fracture
- Significantly diminished range of motion which could be asign of a rotator cuff tear, a dislocation, or fracture
- Severe, persistent, or unrelenting pain that is not relieved with painkillers as this could signify a more serious underlying cause of the symptoms
- Weakness or numbness in arms and hands
- Change in sensation along the arm is a sign which could indicate that the nerves are affected or involved in some way
How Shoulder Pain Is Examined And Diagnosed
While the internet is helpful to understand more about the shoulder joint and pain, a specialized doctor trained in orthobiologics and regenerative treatment options should be involved to get an accurate diagnosis of any symptoms. Avoid clinics and providers that only provide options to mask the pain such as NSAID or steroids.
Commonly, a doctor will examine the shoulder joint in conjunction with the neck, axilla, and chest wall. This is done because these areas share a common muscle, nerve, and blood supply.
They will also inspect the shoulders for any swelling, deformity, or wasting. To look for tenderness, swelling, warmth, and crepitus, they will also likely palpate the sternoclavicular, AC, and GH joints.
Specific exams to compare power, stability, and range of movement including active, passive, and resisted motion of both shoulders should also be completed. The doctor may also assess for a painful arc during abduction of the shoulder and test rotational movements as well.
The drop arm test, apprehension test, and Hawkin’s impingement tests are all completed to assess the integrity or involvement of specific ligaments within the joint.
Imaging is the next step following the physical examination:
- X-ray: Radiographs or X-rays may be needed to further assess the shoulder joint pain, particularly after a fall or accident. The standard x-ray series includes an anteroposterior, scapular Y, and axillary view so that the doctor can see the entire shoulder joint across all planes.
X-rays are also useful to assess osteoarthritis of the AC and GH joints. They can also be used to visualize large rotator cuff tears and calcific tendinitis, Hill-Sachs dislocations, or an avulsion fracture of the glenoid. - MRI: If the diagnosis remains unclear, an MRI might be used to further examine the joint. Soft tissue injuries are commonly assessed with MRI, and the preferred test of choice for rotator cuff injuries is MRI. An MRI can also visualize rotator cuff tendinopathy, partial tears, and complete tears in addition to visualizing and assessing the joint cartilage and shoulder labrum.
- Ultrasonography: This is a cost-effective alternative to MRI. Like an MRI, ultrasonography can aid in the diagnosis of rotator cuff tears.
At the Centeno-Schultz Clinic, an ultrasound evaluation of the shoulder is part of the new-patient evaluation and provides real-time information for patients with shoulder joint pain. - CT: A CT scan is used to assess for bone injuries of the shoulder, including arthritis, erosion of the bone, bone loss of the humeral head or the glenoid, tumors, and hairline or occult fractures.
Arthrography: In this imaging study, the joint is injected with contrast and is assessed with a CT or MRI. CT arthrography is useful to assess suspected rotator cuff tears in patients who cannot undergo an MRI. MRI arthrography is the preferred test when a patient is suspected to have the pathology of the labrum of the joint.
Common Treatments For Shoulder Joint Pain
There are many treatment options for shoulder joint pain. These include medications, acupuncture, surgery, and non-surgical alternatives like regenerative medicine and biological therapy. Below is a detailed explanation for each of these treatment options:
- Medications: Medications, such as painkillers, are used to reduce shoulder joint pain. For example, NSAIDs like ibuprofen are helpful to reduce inflammation and are used to manage acute pain. However, they should not be used for more than two weeks as they can cause gastritis.
If the pain is not controlled with NSAIDs, oral steroids or injections may be recommended by a doctor. Steroids can help reduce inflammation, which in turn relieves pain, but can have long-term, negative side effects.
- Acupuncture: Acupuncture is being increasingly used to treat shoulder joint pain. It is a practice that involves using fine needles at various pressure points to relieve pain.
Its clinical efficacy have been small and limited. A systematic review of the existing scientific studies has not shown any evidence to support or refute acupuncture. However, they did show that acupuncture with mobilization of the shoulder helped improve shoulder function in the short term (3).
- Surgery: If the symptoms are persistent or severe, a doctor may recommend surgery (depending on the cause of the pain).
Surgery may be used to repair a rotator cuff tear, decompress impinged nerves, incise tight joint capsules in case of a frozen shoulder, or to complete a total shoulder joint replacement in the case of a complex fracture or severe arthritis.
These surgeries can take place arthroscopically or through an open procedure. The choice of open or arthroscopic procedure depends on the size and location of the damage and the surgeon performing the procedure.
There are no guarantees with surgery and a patient’s pain may increase or remain the same after shoulder surgery. Other significant risks include bleeding, infection, failure, escalation in pain, nerve damage and shoulder instability.
Rotator cuff repair is associated with a high incidence of re-tears ranging from 13-94% (5).
- Non-Surgical Alternatives: Regenerative medicine is a growing area that can provide an alternative to surgery. Regenerative treatments options include the use of PRP and bone marrow concentrate which, in many cases, can facilitate healing and restore shoulder stability.
At Centeno-Schultz Clinic, our patients have avoided total joint replacements by opting to use their own stem cells to heal torn rotator cuffs and fractures successfully. Regenerative medicine procedures can save your shoulder and eliminate pain.
The first thing our doctors address is the toxic environment within the joint. They work on reducing inflammation and introducing stem cells to repair the tissues, along with introducing nutrients that will promote healing.
The second thing is to improve mechanical function by incremental physical therapy, which is introduced gradually. By using them both, physical therapy will help the joint regain movement as the injury repairs and recovers. This will preserve the function of the shoulder joint.
Another great alternative is platelet-rich plasma (PRP). If there is ligament laxity, PRP injections can be very helpful in strengthening and increasing ligament stability. Some of our patients that have chosen PRP injections for their shoulder joint pain recovered well and have no pain or range of motion limitations.
Learn How To Manage Shoulder Pain
There are many different treatment options for shoulder pain, so it’s important to talk to your doctor to determine what treatment will work best for you.
If you have chronic shoulder pain, ask your doctor about nonsurgical alternatives and regenerative therapy before you finalize a treatment plan with your doctor. If your doctor is not keen on alternative therapies, then get a second opinion before choosing surgery.
Pain in the shoulder joint pain shouldn’t keep you from living a normal life. Request an appointment with one of the world’s experts in the field of Interventional Orthobiologics today.
John Schultz, MD
John R. Schultz M.D. is a national expert and specialist in Interventional Orthopedics and the clinical use of bone marrow concentrate and PRP for orthopedic injuries. He is board certified in Anesthesiology and Pain Medicine and underwent fellowship training. Dr. Schultz has extensive experience with same day as well as culture expanded bone marrow concentrate and sees patients at the CSC Broomfield, Colorado Clinic, as well the Regenexx Clinic in Grand Cayman. Dr. Schultz emphasis is on the evaluation and treatment of thoracic and cervical disc, facet, nerve, and ligament injuries including the non-surgical treatment of Craniocervical instability (CCI).
References
- Urwin M, Symmons D, Allison T, Brammah T, Busby H, Roxby M, et al. Estimating the burden of musculoskeletal disorders in the community: the comparative prevalence of symptoms at different anatomical sites, and the relation to social deprivation. Ann Rheum Dis 1998;57: 649-55.
- Oh JH, Kim JY, Lee HK, Choi JA. Classification and clinical significance of acromial spur in rotator cuff tear: heel-type spur and rotator cuff tear. Clin Orthop Relat Res. 2010 Jun;468(6):1542-50. doi: 10.1007/s11999-009-1058-5. Epub 2009 Sep 4. PMID: 19760471; PMCID: PMC2865608.
- Green S, Buchbinder R, Hetrick S. Acupuncture for shoulder pain. Cochrane Database Syst Rev. 2005;(2):CD005319. Published 2005 Apr 18. doi:10.1002/14651858.CD005319
- Kim GK. The Risk of Fluoroquinolone-induced Tendinopathy and Tendon Rupture: What Does The Clinician Need To Know? J Clin Aesthet Dermatol. 2010 Apr;3(4):49-54. PMID: 20725547; PMCID: PMC2921747.
- Mandaleson A. Re-tears after rotator cuff repair: Current concepts review. J Clin Orthop Trauma. 2021 May 21;19:168-174. doi: 10.1016/j.jcot.2021.05.019. PMID: 34123722; PMCID: PMC8170498.
