The low back pain and spinal curve started gradually. Over time it has progressed such that the pain is now constant and you tilt to one side. Conservative care, medications, and steroids have not helped. Your doctor thinks that you have scoliosis. What is Degenerative Scoliosis? How is it diagnosed? What are the symptoms of Degenerative Scoliosis? How is it measured? Can Degenerative Scoliosis be reversed? What are the treatment options? Are there new non-surgical treatment options for back pain? What is a Percutaneous Scolioplasty? Let’s dig in.
What Is Degenerative Scoliosis?(Curved Spine)
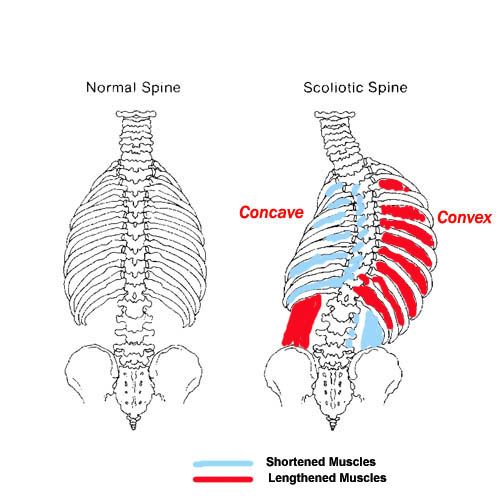
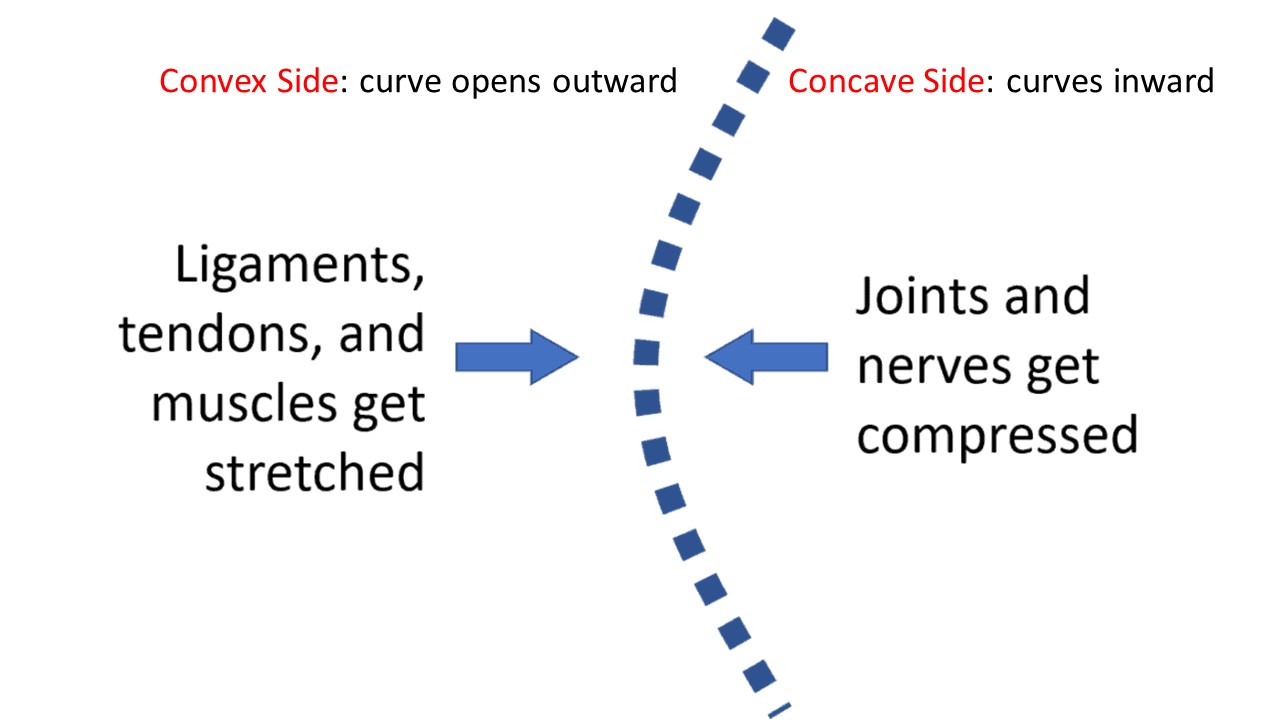
Degenerative Scoliosis, also known as Adult-onset Scoliosis, is a medical condition that involves a side bending in the spine. The bending can be mild, moderate, or severe with side-bending to either the right or the left. The term degenerative means generalized wear and tear and is common as we get older. Degenerative scoliosis is the curvature of the spine that occurs as a result of degeneration of the discs, small joints, and building blocks. The Degenerative Scoliosis curve is often located in the low back and forms a ‘C” shape. There is a convex and a concave side. The convex side is the open side where it curves outward. The concave side is opposite the convex side, is smaller, and curves inward.
Degenerative Scoliosis is not to be confused with adolescent scoliosis commonly seen in adolescents during a growth spurt. This is called Adolescent Idiopathic Scoliosis (1).
How Is Degenerative Scoliosis Diagnosed?
The first step is a complete evaluation by your physician that includes a review of past medical history, trauma, past surgical history, and a list of current medications. A physical examination is essential. Your doctor will examine your posture, walk, symmetry of shoulders and hips along with your ability to bend forward, backward, and twist. Muscle strength and size will be evaluated. Radiographic tests that may be ordered include a full body x-ray, MRI, or CT scan.
What Are the Symptoms of Degenerative Scoliosis? (Pain)
Symptoms, pain, and limitations are dependent upon the duration and severity of Degenerative Scoliosis (2). Some patients may experience no symptoms. In some mild cases, the symptoms are similar to lumbar degenerative disc disease. What is different in Degenerative Scoliosis is that the patients typically report different types of pain on either side of the spinal curve. Some have pain only on one side of the spine whereas others have it on both sides. On the compressed side, the concave side of the spinal curve common symptoms include:
Deep, unrelenting pain in the mid and low back
Electrical, shearing pain in the low back, buttock that radiates down the leg (sciatica)
Tingling and pins and needles in one leg
Mid and low back persistent muscle spasms and weakness
The convex side of the spinal curve has the curve that opens up. Muscles, tendons, and ligaments on the convex side are stretched due to the spinal opening up on this side of the spine. Common symptoms include:
Persistent muscle tightness that does not respond to conservative treatment
Enlarged muscles on this side of the spine as they are constantly being pulled
Symptoms are not acute and progress gradually over time. They are typically worse first thing in the morning and improve with activity and as the day progresses.
Big Toe Numbness
Believe it or not, one of those significant issues that can present as numbness stems from the low back. In the lumbar spine, the nerve that exits the spine at the L5 level branches down through the hip, thigh, knee, lower leg, and, yes, all the way into the foot and toes. So a pinched or irritated nerve at that L5 level in the back can create problems, such as pain, numbness, tingling, and so on, anywhere along the nerve branch. So what can irritate the L5 spinal nerve? The list is long, but it includes disc issues, such as herniated…
Throwing this question out to the social-media masses is sure to bring out the cyber “comedians” among us, but the truth is when you really do have butt pain, it’s no laughing matter. So we’re glad you came here to ask because we actually do see many patients in our clinic with this problem. There are a number of issues that can cause butt pain, but the root causes we most often discover are hamstrings tendinopathy, a pinched low-back nerve, or sacroiliac joint syndrome. Let’s take a look at each of these individually. – Hamstrings Tendinopathy: The hamstrings are actually a collection of large muscles…
A twitching calf muscle may seem like no big deal, and if it’s just a temporary annoyance that lasts a couple of days and then goes away, it may be. However, it can also be a warning sign of something bigger, especially if it continues. So, today, we’re going to explain a little about the calf and why it’s not a good idea to ignore calf muscle twitching. If there’s one muscle you’re likely familiar with, it’s the calf muscle. If you reach around and grab your calf and flex it, the muscle you are actually feeling just under the surface is called the gastrocnemius muscle.
The gluteus medius is one of the major muscles in your buttock and hip. There are three gluteal muscles you have probably heard about: They layer one upon the another much like a layer cake. The gluteus minimus is closest to the body followed by the gluteus medius and then the larger gluteus maximus.Gluteus Minimus – The gluteus minimus is the smallest of the three gluteal muscles. It is a small triangular muscle that lies underneath its bigger brother, the gluteus medius. It functions to stabilize the hip, rotate the thigh, and move the hip in an outward direction.Gluteus Medius -A powerful muscle that starts at the backside of your waist bone…
So what exactly causes the leg to feel disconnected? The hip joint is the connection point between the leg and the rest of the body. The femur in the leg and the acetabulum in the pelvis create the hip joint. So if the left SI joint, for example, in the back and the symphysis pubis joint in the front becomes unstable due to loose supporting ligaments, then the left leg, which is connected between the two joints, is likely to also feel a bit disconnected. Likewise, if the right SI joint were unstable, then the right leg might feel disconnected. How This Patient’s “Disconnected” Leg Was Fixed Despite “leg feels…
Have you ever been walking and your leg gives out? It can be both surprising and alarming What would cause your leg to give out? Can sciatica cause your leg to give out? How do you treat weak legs? Let’s dig in.Weakness in the leg can arise from three principal sources: nerve problems, muscle weakness, and SI joint dysfunction. Weakness in the legs may indicate a significant nerve problem. In many cases, it may be the first indication of a nerve problem. There are three common causes of nerve injury: low back disorders, nerve compression as it descends down into the hip, thigh, and shin and medical conditions such as diabetes…
After a long day on your feet sitting down is supposed to be way to relaxing. Unfortunately for some sitting for any length of time can be painful. Most people experience low back pain at some point in their life. The lifetime prevalence of low back pain is 85% (1). Let’s take a deeper look at the different types of pain and causes of low back pain when sitting.
Pain can present in many different ways. It can be intermitent or constant. The quality of the low back pain can also vary depending upon the actual source of injury. Common examples include:
Sharp and Stabbing, Dull and Aching, Throbbing/ Pulsating, Pins and Needles, Burning, Electrical
When you’re seated, the facet joints in your lower back are in an open and slightly flexed position. When you stand up, these joints compress. If they are painful or have arthritis, you’ll have pain as you stand up because this puts pressure on the painful joints. In addition, if there is any type of movement of one vertebra forward on another (called spondylolisthesis), then this shift will have occurred as you sit. This is called degenerative spondylolisthesis. When you get back up, the vertebrae will come back into position after a few seconds, leading to that awkward “walk it out period” that starts out painful and ends up more normal.
The thoracic spine is the part of the spine below the neck (cervical spine) and above the low back (lumbar spine). It is often referred to as the mid back. Nerves exit the thoracic spine at each level and can become irritated, compressed or injured, resulting in pain and dysfunction. This is commonly referred to as thoracic radiculopathy or pinched nerve.
The hamstrings are a group of muscles in the upper leg. They are located on the backside of the upper leg and are comprised of three muscles: biceps femoris, semitendinosus, and semimembranosus. The calf muscles are located on the backside of the lower leg and are comprised of two muscles: the gastrocnemius and soleus. Tight hamstring and calf muscles can be painful, limiting someone mobility. They also make lower extremity muscles more vulnerable to injuries. Tight hamstrings and calves can arise from different sources which include: medication, muscle and tendon injury, overuse, muscle imbalance, dehydration, poor posture, low back injury…
Upper back pain between the shoulder blades is also known as interscapular pain. Fifteen percent of the population suffers from chronic upper back pain. Finding the source of interscapular pain can be tricky because the upper back houses many important structures like the heart, the upper lobes of the lung, the cervical spine, the scapulas, and a dozen or so of muscles and nerves.
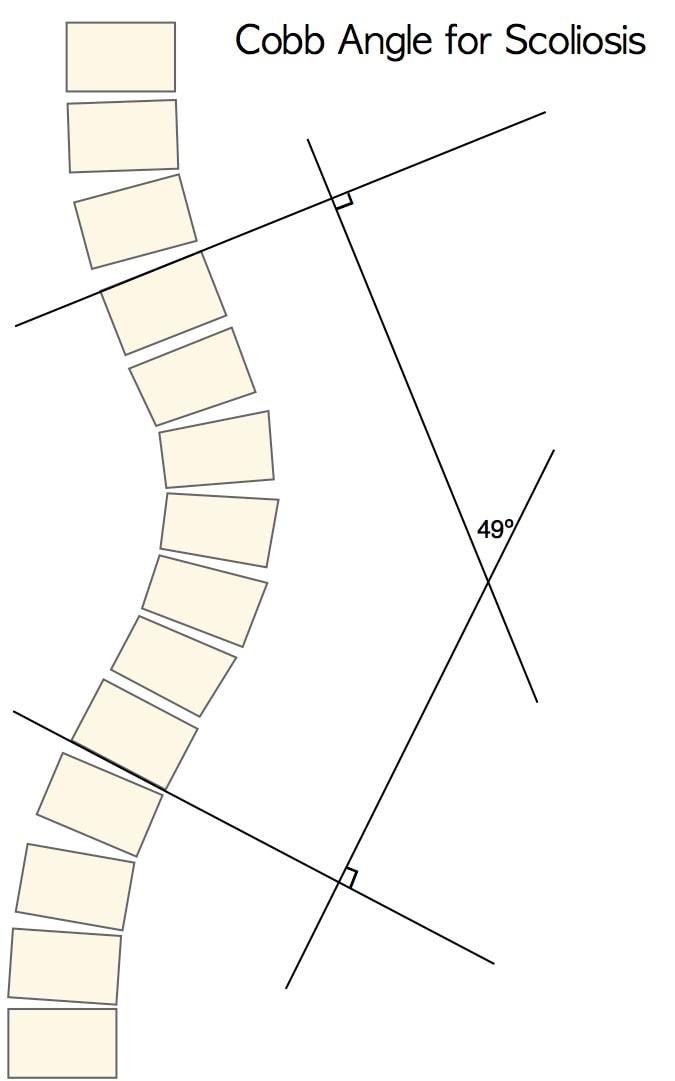
The Cobb angle is a measure of the curvature of the spine. It is the most widely used measurement to quantify the magnitude of spinal deformities. It is measured in degrees. Scoliosis is defined as a lateral spinal curvature with a Cobb angle of >10° (3)
How is the Cobb angle measured? As shown here, this is the angle formed between lines drawn parallel to the vertebra at the beginning and end of the curve. The treatment type chosen for the Scoliosis patient is often determined by this angle:
Scoliosis-specific exercises (15 – 25° Cobb)
Bracing (20 – 40° Cobb)
Spinal fusion surgery (> 40 – 50° Cobb)
For smaller curves exercise therapy is often prescribed. For medium curves measuring between 20-40 degrees bracing is used. Finally, in severe curves measuring in excess of 40 degrees, spinal fusion surgery is often utilized. As discussed later in the post, we have a new treatment option involving Interventional Orthobiologics that may make surgery less common.
Can Degenerative Scoliosis Be Reversed?
The short answer is no. The severity of Scoliosis will determine the appropriate course of action. Certain types of injections discussed below may slow the progression of Scoliosis. Once the curve in the spine has started the only way to try to straighten the spine would be by using fusion surgery with long rods. However, straightening a young spine where the bones have yet to change shape is easier. In Degenerative Scoliosis, the shape of the bones has already changed, so there is really no practical way to straighten the spine, even with surgical fusion.
What Is the Treatment for Degenerative Scoliosis? (Conservative Care, Injections and Surgery)
Treatment for Degenerative Scoliosis will depend upon the severity of the spinal curve, symptoms, underlying medical conditions, and one’s overall level of functioning. When appropriate conservative care should always be first-line treatment. The three principal treatment options include:
Conservative Care
Treatment options include physical therapy, massage, dry needling, stretching, chiropractic care, and targeted exercise. Exercises are can be effective in the treatment of some cases of Degenerative Scoliosis. The most popular physical therapy to avoid scoliosis surgery is the Schroth method which was founded in the 1920s. This involves pelvic corrections, right angular breathing, and stretching/strengthening to stabilize and correct the spine (4). High-quality studies have shown that this can be effective long-term in reducing the Cobb angle (5). In addition, long-term follow-up studies have shown that AIS patients treated with either bracing or surgery had little difference in the quality of life (6).
Traditional Pain Injections
High-dose steroid epidural injections are commonly used for patients with Degenerative Scoliosis. The procedure is performed at a pain clinic or ambulatory surgery center. The goal is to reduce the inflammation and irritation of the spine and exiting nerves. Facet joint steroid injections are also used with the goal of reducing the inflammation and pain in the facet joint. Facet joints are small paired joints on the backside of the spine that provides stability and limit rotation. In Degenerative Scoliosis, they can be injured or irritated as a result of the curve in the spine. While steroids are very effective anti-inflammatory agents they cause extensive damage to orthopedic tissue. The very steroids that are injected into the epidural space and facets have been demonstrated to be toxic to muscles, tendons, and ligaments and destroy cartilage (7).
Surgery
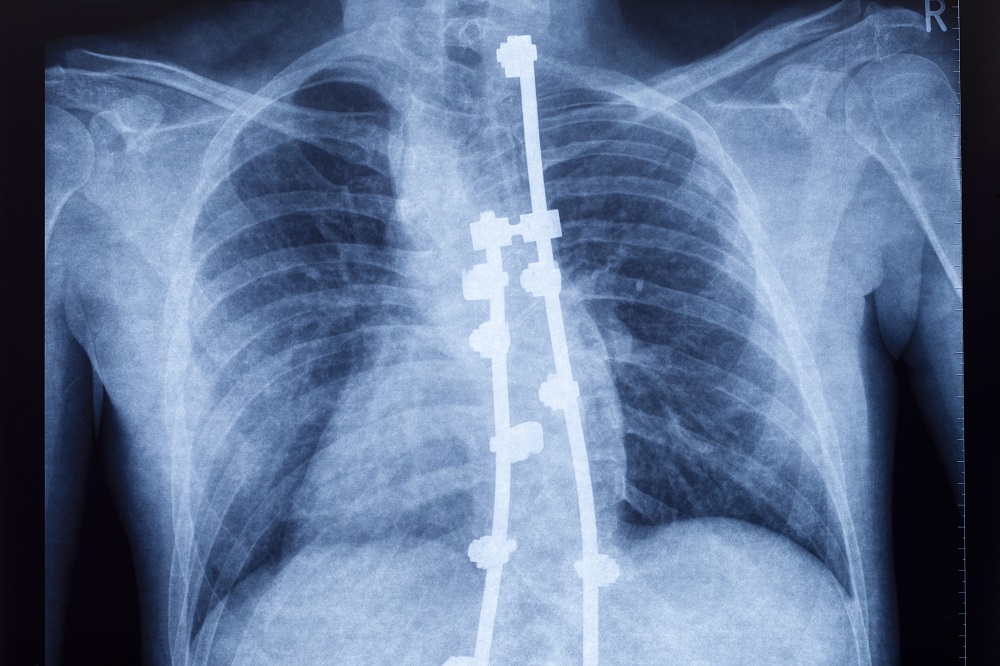
Surgery treatment typically involves multi-level fusion. Fusion is a surgical procedure where one or more of the spinal building blocks (vertebral bodies) are joined together, straightened, and stabilized by screws, bolts, and rods. Degenerative Scoliosis surgery is a major surgery requiring many hours and extensive rehabilitation. There are significant risks that include bleeding, infection, failure, escalation in pain, nerve damage, failed fusion, Complex Regional Pain Syndrome (CRPS). In addition, patients are at risk for additional degeneration of the discs, facet, and ligaments above and below the fusion. This is called Adjacent Segment Disease. To learn more about this significant complication please click on the video below.
A New, Non-surgical Approach to Treating Degenerative Scoliosis
When the spine side bends, there is one side that’s compressed and one side that gets stretched. Hence, on the side of the compression (the concave side), the joints and holes for the nerves (foramina) get extra forces which cause the joints to become big and arthritic and the spinal nerves to become irritated leading to sciatica. On the side of the stretching (convex side), the tendons, ligaments and muscles get pulled on which leads to them getting beat up.
While the traditional pain management approaches above focus on finding one thing that’s causing pain, in Degenerative Scoliosis, it’s often many things that are causing pain. Hence, we developed a procedure that uses precise Orthobiologic injections into many structures. The procedure is called a Percutaneous Scolioplasty. So on the side of the concavity, we’re injecting into many facet joints and nerve areas that are getting compressed and on the side of the convexity, we’re injecting into all of those beat-up tendons and ligaments. Orthobiologics are things like platelet-rich plasma or bone marrow concentrate which contains stem cells that may help these areas heal. The goal of using precise Orthobiologic injections is to:
Tighten and strengthen tissues that are under stress due to a curve in the spine
Reduce deformity and provide additional resistance to further collapse
Reduce irritation of spinal nerves, small joints, tendons, and ligaments on the convex side of the curve
Reduce the pain and dysfunction originating from areas of tendon injury on the concave side of the curve
Improve the ability of the multifidus to stabilize the spine
Functional Degenerative Scoliosis Treatment
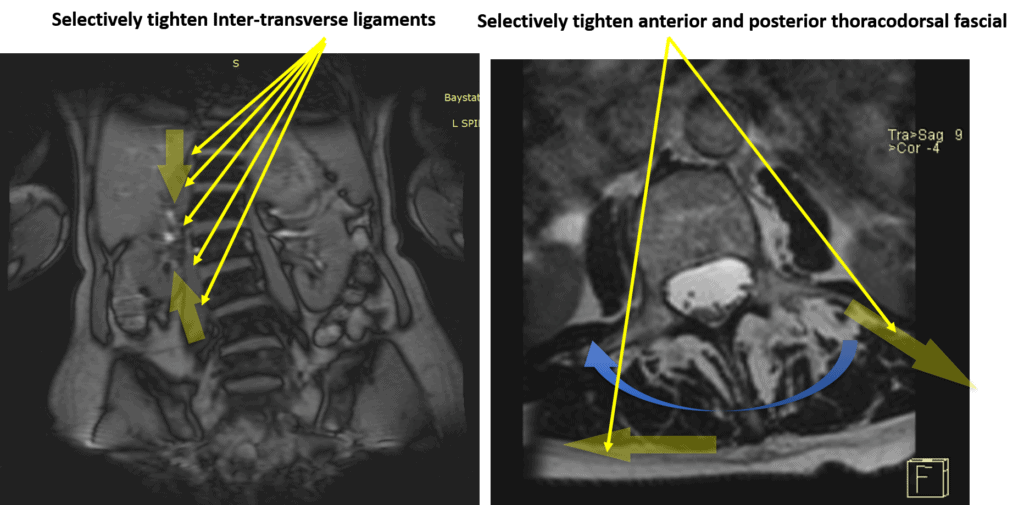
The problem with Scoliosis is that the farther its side is bent off-center, the more it wants to move in that direction. So while helping areas that hurt is great, what if we could buttress the ligaments and fascia in a precise way to provide support for the scoliosis? That’s the second part of this new procedure. These same Orthobiologics can be used in a precise injection to target and tighten the ligaments and fascia.
For example, the above image on the left is an MRI of the lumbar spine that mildly bends to the left. It is a frontal image (coronal). There are important ligaments between the spinal building blocks called Inter-Transverse Ligaments. In degenerative scoliosis, these ligaments are stretched on the convex side (the side with the curve that opens up). These ligaments can be injected under x-ray or ultrasound guidance. The goal of the injection is to tighten the stretched Interspinous Ligaments thereby limiting the progressive spinal curve and associated symptoms.
The above image on the right is a side cut of the lumbar spine otherwise known as an axial image. The large boney prominence that you can feel when you touch someone’s back is rotated to the right. This is consistent with Degenerative Scoliosis as when the spine side bends it also rotates. In this case, the supporting fascia and ligaments can be injected to reduce the spine’s rotation. A key supporting structure is which is identified by the blue arrows is the Thoracolumbar Fascia. It is treated with PRP or bone marrow concentrate which contains stem cells in an effort to restore spinal alignment.
To learn more about Percutaneous Scolioplasty, see the video below:
In Conclusion
Degenerative Scoliosis, also known as Adult-onset Scoliosis, is a medical condition that involves a side bending in the spine.
One side of the spine curve is open and is called the convex side. Directly opposite the convex side, the spinal curve turns inward which is called the concave side. The result is a C shaped curve.
Degenerative Scoliosis is not to be confused with Adolescent Scoliosis.
Degenerative Scoliosis is diagnosed by physical examination, review of medical history, and radiographic studies.
Symptoms vary depending upon the duration and severity of Degenerative Scoliosis.
Symptoms may involve one side of the spine or both,
The Cobb angle is a measure of the curvature of the spine. It is measured in degrees.
Degenerative Scoliosis can be successfully managed but not reversed.
Treatment options include conservative care, traditional pain injections, and surgery.
Degenerative Scoliosis surgery is major surgery with extensive rehabilitation and a list of complications including failure.
Percutaneous Scolioplasty is a nonsurgical treatment option utilized exclusively at the Centeno-Schultz Clinic where PRP and bone marrow stem cells are injected in areas of damage to decompress the overloaded, injured tissue and improve symmetrical stability.
If you or a loved one has Degenerative Scoliosis with pain and limitations please schedule a telephone candidacy discussion with a board-certified, fellowship-trained physician. From the comfort of your home, office or beach cottage learn what treatment options are available for you. Call today and stop the pain, misery, and suffering. Act now before you become dependent upon medications or you find yourself in a surgeon’s office desperate for relief.
Laminectomy
A laminectomy is a surgical procedure designed to relieve pressure on the spinal cord or nerves by removing a portion of the vertebral bone called the lamina. This procedure is typically performed to alleviate symptoms caused by spinal stenosis, herniated discs, or other conditions that result in spinal nerve compression. By removing the lamina, the spinal canal is widened, reducing pressure and providing relief from pain, numbness, and weakness. This surgery is often recommended when conservative treatments, such as physical therapy and medication, have not provided sufficient relief.
Prolotherapy is an injection based regenerative therapy used in the treatment of ligament, tendon, muscle and spine injuries. It is minimally invasive and involves the injection of an irritant such as dextrose into the damaged or painful area. The injected irritant stimulates a delayed or frozen healing cycle thereby increasing blood flow and tissue healing. The thoracic spine is that section of the spine that is below the neck and above the low back. It is also referred to as the mid back. It has multiple components that include: Vertebral Bodies: Boney building blocks that stack one upon another…
PRP is short for platelet-rich plasma, and it is autologous blood with concentrations of platelets above baseline values. The potential benefit of platelet-rich plasma has received considerable interest due to the appeal of a simple, safe, and minimally invasive method of applying growth factors. PRP treatments are a form of regenerative medicine that utilizes the blood healing factors to help the body repair itself by means of injecting PRP into the damaged tissue. In regenerative orthopedics, it is typically used for the treatment of muscle strains, tears, ligament and tendon tears, minor arthritis, and joint instability. There have been more than 30 randomized controlled trials of PRP…
Thoracic spine surgery is a major surgery aimed at treating injuries in the thoracic spine. Because of the complex anatomy and close proximity to the heart and lungs, there are significant surgical risks and complications. Surgery on the thoracic spine can take hours and may require deflating the lung in order to gain access to the thoracic injury. Recovery can be lengthy depending upon the specific thoracic spine surgery performed. There are several different types of thoracic spine surgery. The specific thoracic spine performed depends upon the underlying thoracic injury and a symptoms of the patient. For example, a thoracic disc herniation…
Transforaminal Lumbar Interbody Fusion is a variant of the Posterior Lumbar Interbody Fusion (PLIF) technique described by Cloward in the 1950s. PLIF has been associated with the high incidences of neurological complications, up to 13.6% of permanent neurologic lesions in Barnes’ et al. study, in particular of the traversing nerve root (2,3) This is due to the fact that a great amount of traction on the dural sac is required to implant the interbody fusion devices. Surgeons have transitioned to TLIF in efforts to reduce complication rates. Success rates vary depending on what literature you read and recently all orthopedic surgery literature has come under fire…
Christopher J. Centeno, M.D. is an international expert and specialist in Interventional Orthopedics and the clinical use of bone marrow concentrate in orthopedics.
Dr. Centeno is one of the few physicians in the world with extensive experience in the culture expansion of and clinical use of adult bone marrow concentrate to treat orthopedic injuries. His clinic incorporates a variety of revolutionary pain management techniques to bring its broad patient base relief and results. Dr. Centeno treats patients from all over the US who travel to Colorado to undergo innovative, non-surgical treatments. Dr. Centeno has chaired multiple international research-based conferences. He also maintains an active research-based practice, with multiple publications listed in the US National Library of Medicine. Dr. Centeno has also served as editor-in-chief of a medical research journal dedicated to traumatic injury.
Dr. Centeno trained at the Baylor College of Medicine, Texas Medical Center, and the Institute for Rehabilitation Research. He hails from both Florida and New York and currently resides in Boulder, Colorado with his wife and three children.
John R. Schultz M.D. is a national expert and specialist in Interventional Orthopedics and the clinical use of bone marrow concentrate for orthopedic injuries. He is board certified in Anesthesiology and Pain Medicine and underwent fellowship training in both. Dr. Schultz has extensive experience with same day as well as culture expanded bone marrow concentrate and sees patients at the CSC Broomfield, Colorado Clinic, as well the Regenexx Clinic in Grand Cayman. Dr. Schultz emphasis is on the evaluation and treatment of thoracic and cervical disc, facet, nerve, and ligament injuries including the non-surgical treatment of Craniocervical instability (CCI). Dr. Schultz trained at George Washington School of…
Dr. Pitts is originally from Chicago, IL but is a medical graduate of Vanderbilt School of Medicine in Nashville, TN. After Vanderbilt, he completed a residency in Physical Medicine and Rehabilitation (PM&R) at Emory University in Atlanta, GA. The focus of PM&R is the restoration of function and quality of life. In residency, he gained much experience in musculoskeletal medicine, rehabilitation, spine, and sports medicine along with some regenerative medicine. He also gained significant experience in fluoroscopically guided spinal procedures and peripheral injections. However, Dr. Pitts wanted to broaden his skills and treatment options beyond the current typical standards of care.
Post-residency, Dr. Markle was selected to the Interventional Orthopedic Fellowship program at the Centeno-Schultz Clinic. During his fellowship, he gained significant experience in the new field of Interventional Orthopedics and regenerative medicine, honing his skills in advanced injection techniques into the spine and joints treating patients with autologous, bone marrow concentrate and platelet solutions. Dr. Markle then accepted a full-time attending physician position at the Centeno-Schultz Clinic, where he both treats patients and trains Interventional Orthopedics fellows. Dr. Markle is an active member of the Interventional Orthopedic Foundation and serves as a course instructor, where he trains physicians from around the world.
Dr. Money is an Indiana native who now proudly calls Colorado home. He attended medical school at Kansas City University and then returned to Indiana to complete a Physical Medicine and Rehabilitation residency program at Indiana University, where he was trained on non-surgical methods to improve health and function as well as rehabilitative care following trauma, stroke, spinal cord injury, brain injury, etc. Dr. Money has been following the ideology behind Centeno-Schultz Clinic and Regenexx since he was in medical school, as he believed there had to be a better way to care for patients than the status quo. The human body has incredible healing capabilities…
Back pain is a common complaint among golfers, impacting both amateur enthusiasts and professional athletes. Golf, while seemingly low-impact, involves repetitive, high-intensity movements that can stress the spine and surrounding structures. Understanding the causes, symptoms, and preventative measures for golf-related back pain can help maintain performance and long-term health. Golf And Back Pain The golf…
Navigating spinal fusion recovery can be a daunting prospect, given its impact on daily life and mobility. Understanding what to expect during this process is crucial for individuals undergoing this procedure. In this article, we’ll explore the typical timeline, challenges, and strategies for managing recovery after spinal fusion surgery, providing insights to help individuals prepare…
Back cracking is a phenomenon that many people experience, often eliciting both curiosity and concern. Whether it’s the satisfying pop from a morning stretch or the deliberate twist during a yoga session, the sound and sensation of cracking your back can be oddly gratifying. But what exactly is happening inside your body when you hear…
Spinal fusion, also known as back fusion, is a surgical procedure designed to help severe spinal instability that causes severe pain or nerve injuries. It involves permanently connecting two or more vertebrae in your spine to eliminate motion between them. This article will delve into the intricacies of spinal fusion, exploring the reasons behind the…
The human spine, a marvel of engineering, is not a straight column but rather a structure with gentle curves. These natural curves are essential for maintaining balance, allowing flexibility, and absorbing the shock of movement. The spine’s curvature plays a critical role in overall health, influencing posture, mobility, and the function of the nervous system. …
Have you had a neck injury or whiplash trauma? Do you have neck pain, especially when looking up, and you don’t know the cause? Then you may want to learn about the cervical anterior longitudinal ligament (ALL). Anatomy of the Anterior Longitudinal Ligament The ALL is a strong, wide ligament that runs along the front…
5.Schreiber S., Parent E.C., Khodayari Moez E., Hedden D.M., Hill D.L., Moreau M., Lou E., Watkins E.M., Southon S.C. Schroth physiotherapeutic scoliosis-specific exercises added to the standard of care lead to better Cobb angle outcomes in adolescents with idiopathic scoliosis – an assessor and statistician blinded randomized controlled trial. PLoS One. 2016;11(12):e0168746. doi: 10.1371/journal.pone.0168746.
6.Andersen M.O., Christensen S.B., Thomsen K. Outcome at 10 years after treatment for adolescent idiopathic scoliosis. Spine. 2006;31(3):350–354. doi: 10.1097/01.brs.0000197649.29712.
7.Wernecke C, Braun HJ, Dragoo JL. The Effect of Intra-articular Corticosteroids on Articular Cartilage: A Systematic Review. Orthop J Sports Med. 2015;3(5):2325967115581163. Published 2015 Apr 27. doi:10.1177/2325967115581163
Ready to get help for your Degenerative Scoliosis?