Your low back and buttock pain has been unrelenting. Your doctor thinks you injured your sacroiliac joint. What is the Sacroiliac Joint? What is SI Joint Surgery? How successful is SI joint surgery? What are the complications of SI joint surgery? What is SI joint fusion? How can I successfully treat the SI joint without surgery? Let’s dig in.
Sacroiliac Joint (SI)
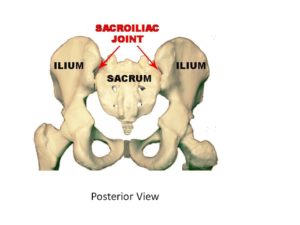
The sacroiliac (SI) joint is a very important joint in the lower back. It is formed by the tailbone (sacrum) and waist bones (ilium) and functions as a shock absorber between the spine and legs. It is a C shaped joint with cartilage and an extensive complex of supporting ligaments. Each of us has two sacroiliac joints. One on the left and one on the right. SI joint pain is common with an incidence of 15-30% of patients with low back pain (1).
SI Joint Referral Pattern
One of the functions of the SI joint is a shock absorber. It transfers the forces from the upper body to the lower body. As such it is susceptible to injury which can impact its ability to act as a shock absorber. Causes of SI joint injury include trauma, degeneration, inflammation, pregnancy, ligament laxity, and muscle weakness (2). Patients that have undergone lumbar fusions are particularly susceptible to SI joint injury. A recent study reported that up to 75% of patients who undergo lumbar fusion will develop SI joint degeneration (3).
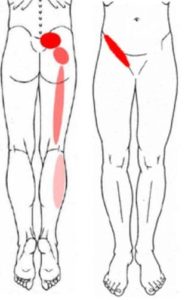
Pain is the most prominent symptom and typically involves the dimples of Venus (4). One-sided low back and buttock pain is common and typically made worse with sitting and transitioning from the sitting to standing position. If severe, the pain can radiate into the buttock, posterior thigh extending down to the calf.
SI Joint Surgery
The most common surgery used to treat SI joint pain and instability is SI joint fusion. The surgery involves placing screws or other hardware across the SI joint. This allows the ilium and waist bones to grow together (fuse) A new system called the IFuse uses a titanium implant that is placed across the joint. The surgery requires general anesthesia and takes 1-2 hours.
How Successful Is SI Joint Fusion?
SI joint fusion is a major surgery where large screws or implants are placed across the joint thereby eliminating motion. Please remember that the SI joint is a critical shock absorber between the spine and legs and as such must be able to move. Fusion prevents this function and in doing so can give rise to a number of complications. Success varies dependent upon the surgical technique used and the parameter included in the study. Complications however are significant.
In one study that followed 469 patients for 7 years. There were significant complications which included (5).
Re-operation rates after open surgery ranged from 0%-65% whereas in the minimally invasive surgery re-operation rate ranged from 0-17%.
Major complications ranged from 5%-20% and in one study were found to be 56%.
Continued pain with the need for oral narcotics (8)
Adjacent Segment Disease
Another randomized controlled study (RCT) followed patients for two years after SI joint fusion (8). Results are questionable as 55% of the patients were still taking narcotics two years after the procedure.
SI Joint Surgery Complications
Every surgery is associated with potential risks and complications. Risks include bleeding, infection, escalation in pain, nerve, and muscle damage. Three Important complications you need to know about SI joint Surgery are failure to fuse, failure to relieve the pain, and adjacent segment disease.
Failure to Fuse
Despite screws or inserted implants, the bones may not fuse together creating instability and pain.
Failure to alleviate ongoing pain.
Why? The WRONG DIAGNOSIS! The pain was not arising from the SI joint in the first place. Accordingly, SI joint surgery did not address the source of pain and the patient is left with ongoing pain and compromised gluteal muscles and ligaments that were traumatized during the SI joint surgery.
Adjacent Segment Disease.
This occurs as a result of removing the shock-absorbing properties of a joint or disc. It can occur with any spinal fusion or SI joint fusion. The forces that would normally be absorbed by a given disc or joint are then redirected above and below the affected joint. This means for patients with SI joint surgery, additional pressure will be applied to the lowest lumbar disc and facet joints. These structures in turn become overloaded, injured, and a source of pain. To learn more about adjacent segment disease please click on the video below.
How Do You Fix a Sacroiliac Joint?
At the Centeno-Schultz Clinic, we are experts in the treatment of Si joint injuries. We have extensive experience evaluating and successfully treating SI joint injuries that failed other therapies. Conservative care is always first-line therapy. This may include physical therapy, manual manipulation, SI belts, and gluteal strengthening. Steroid injections are very effective anti-inflammatory agents that must be avoided as they are toxic to the SI joint cartilage and can weaken ligaments (9).
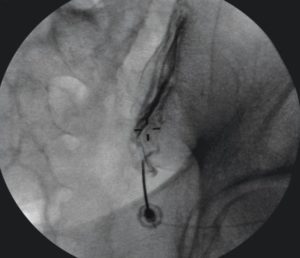
X-ray image of contrast in the right SI joint
There are three important components in the successful evaluation and treatment of SI joint injuries.
Evaluating and treating the SI joint cartilage. This is accomplished by injecting directly into the joint itself. The SI joint can be very difficult to inject. At the Centeno-Schultz Clinic, we have mastered and published a successful injection technique (10). To confirm accurate needle placement contrast is used and needs to be seen within the joint itself as demonstrated in the x-ray to the right.
Evaluating and treating the SI joint ligaments. Ligaments are thick bands of connective tissue that connect one bone to another. They provide important stability for the joint. At the Centeno-Schultz Clinic ligament, evaluation and treatment are the standard of care. Ligaments are easily identified and injected under ultrasound.
Evaluating and treating the muscles which support and stabilize the Si joint. Muscle strength and function is critical for optimal SI joint function.
At the Centeno-Schultz Clinic PRP and stem cells have been used extensively in the successful treatment of SI joint injuries. PRP is rich in growth factors that can increase blood flow and reduce inflammation. Stem cells are a powerhouse of healing that can accelerate recovery. PRP and stem cell treatment allow patients to avoid tissue trauma, extensive downtime, and complications associated with SI joint surgery.
In Conclusion
The SI joint is an important joint in the lower back. It is formed by the tailbone (sacrum) and waist bones (ilium) and functions as a shock absorber between the spine and legs. Injury to the SI joint can be caused by trauma, degeneration, inflammation, pregnancy, ligament laxity, and muscle weakness. Pain is the most prominent symptom. SI joint fusion is the most common SI Joint Surgery to treat SI joint pain and instability. Fusion is major surgery and eliminates motion across the joint. Complications are significant and include failure to fuse, failure to relieve pain, and adjacent segment disease. Successful treatment of SI joint injures involves the treatment of the joint cartilage, supporting ligament and muscles. PRP and stem cells are an effective, safe, natural alternative to SI joint surgery. PRP and stem cells allow patients to avoid the downtime and complications associated with surgery.
If you suffer from ongoing SI joint pain and want to avoid life-threatening surgery please schedule a Telemedicine evaluation. A board-certified, fellowship-trained physician will discuss which treatment is best for you. Act now and say goodbye to your pain and limitations.
To answer this question, fill out the candidate form below to request a new patient evaluation, and a patient advocate will reach out to you to determine your next steps. Your one-hour, in-office or telemedicine evaluation will be with one of the world’s experts in the field of Interventional Orthopedics.