BT is a 36y/o nurse s/p MVA with a five-year history of right upper neck and headache pain which was constant in duration, 6/10 in severity, exclusively right-sided localized principally at the base of her skull with radiations into the back of ther head and forehead. Pain was sharp, stabbing and aching in character and aggravated by extension and stress. BT was a restrained driver of a mini-van when a 18 wheeler truck struck the driver’s side of her vehicle. Treatment to date had included physical therapy, massage, cervical traction, trigger point injects, TENS unit, Botox injections complicated by cervical weakness and radiofrequency ablation of the right C2-4 joints without significant relief. BT was no longer able to work due to her unrelenting pain.
Physical examination was significant for sensitivity to light, balance disturbance preventing her from walking heel to toe, extreme tenderness over the right C0/C1 and C1/2 joint with marked restriction in extension and rotation secondary to pain.
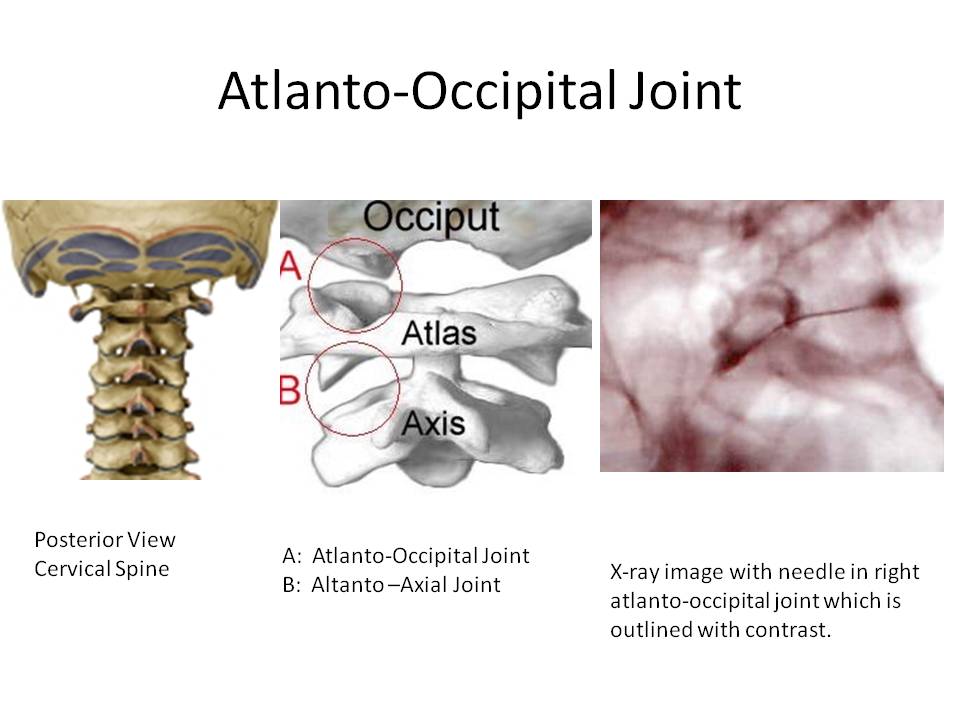
Upper cervical joints are common sources of pain following motor vehicle accidents. The atlanto-occipital joint ( C0/C1) is compromised of the atlas of the vertebral column and the occipital bone (base of skull). The atlas is the topmost (first) cervical vertebra and forms the joint that connect the skull to the spine.
Injection of the right atlanto occipital joint provided 90% reduction in pain. The C0/C1 joint should always be considered as a possible pain generator when evaluating patients with headache pain following motor vehicle accidents. Dreyfuss has mapped the referral patterns. Ogoke was detailed the anatomy, clinical presentation and various treatment modalities.