The other day I was evaluating a patient and reviewing the treatment options for their spine condition. After discussing prior treatments, we got to the topic of medications taken for pain relief. She explained that she mainly utilized anti-inflammatory (NSAID) medications and then she told me to hold how much she takes and has been for many years…..she takes close to 2 grams (2000 milligrams) on a daily basis which equated to about 9-10 capsules of medication per day. I was shocked, considering she was pre-diabetic and with high blood pressure plus the kicker of it is that her PCP (primary care physician) is ok with this. Since this patient wasn’t very aware of the potential side effects of NSAIDs, she is not alone, so I put together the following, the top 5 things you should know about NSAIDs…enjoy.
HOW DO NSAIDs WORK?
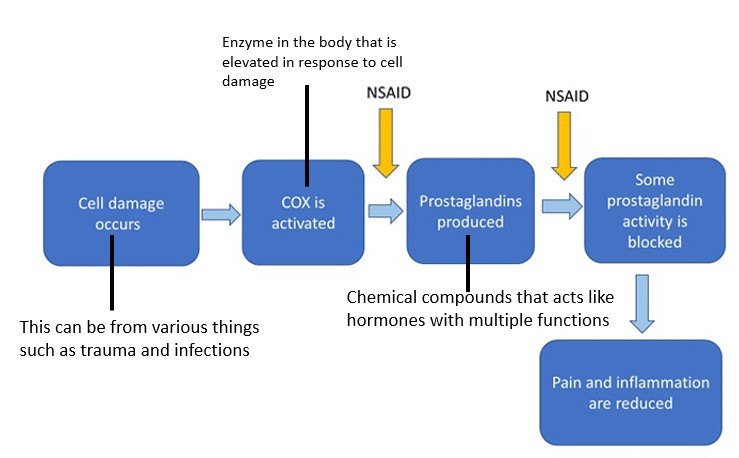
To determine the top 5 things you should know about NSAIDS, we need to first understand how NSAIDs actually work, and then despite the fact that you may feel better when taking them, specifically how and why the risk vs benefit profile actually makes them dangerous. Follow the chart below through the process.
What Are the Top 5 Things You Should Know About NSAIDs?
Nonsteroidal anti-inflammatory drugs (NSAIDs) might possibly be the number one medication worldwide, with more than 70 million prescriptions written each year and 30 billion doses of NSAIDs being consumed annually in the United States alone. These drugs have become the first-line defense for the general public for any and all aches and pains. But is there a downside to them that the drug companies aren’t telling you? Let’s dig in…
#1: NSAIDs Block Inflammation Which Helps Pain and Swelling
To simplify, any trauma that happens to orthopedic tissue (tendon, ligament, cartilage, bone or muscle) stimulates an immune response that brings inflammation and causes localized pain. This is known as the inflammatory response. NSAIDs function to reduce this and effectively reduce the local swelling and pain. Here is a simple diagram illustrating this concept. NSAIDs act on enzymes called cyclo-oxygenase enzyme (COX) and inhibit their action in creating another compound called prostaglandins(PG) (1). NSAIDs are COX inhibitors and therefore reduce the production of PGs and this is reduces the local swelling and pain experienced with injuries.
What are some common anti inflammatory medications?
Ibuprofen
Aspirin
Aleve
naproxen
Naprosyn
Mobic
Meloxicam
Celebrex
Diclofenac
Indomethacin
#2: NSAIDs Inhibit Healing By Blocking Inflammation
Should NSAIDs be taken to reduce pain for fractures?
The majority of the abundant experimental data suggest that NSAIDs delay fracture healing (2-3)! Experts guess it is because of the pivotal role PGs play in allowing fractures to heal properly. Here is a diagram highlighting the roles of PGs in fractures. In this experimental study (https://www.ncbi.nlm.nih.gov/pubmed/12054171), the author was able to demonstrate that specialized NSAIDs such as Celebrex (COX-2 specific inhibitor) was far worse in delaying fracture healing rates as compared to non-specific COX inhibitors such as indomethacin or Tylenol in rats (4).
Clinical studies have demonstrated the risk of non-union fractures (non-union = non-healing fractures)
Deguchi demonstrated that patients after spinal fusion had only a 37% success rate of spine fusion if taking NSAIDs prior to surgery compared to the 93% success rate of those who were not on NSAIDS previously (5).
Glassman compared 300 patients who underwent spinal fusion. 4% of the 121 patients developed non-union who did not take NSAIDs compared to 17% of the 164 patients that were taking NSAIDs(6).-
Bhattacharyya looked at 10,000 patient with femur fractures that underwent surgery and found a 3.7-fold increased risk of non-union in femur fractures when taking NSAIDs (7)
** but large controlled clinical trials are needed to better assess the orthopedic effects of these drugs, and to characterize the patients at clinically significant increased NSAID‐related risk for delayed fracture healing **
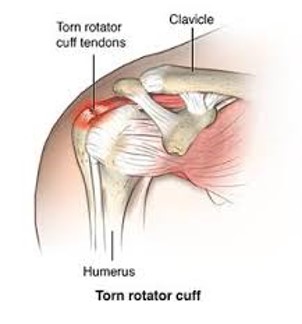
What About Tendon or Ligament Injury?
The healing of a tendon or ligament after injury is a complex process and disrupting any aspect can lead to long-term issues with the function of the ligament or tendon. There are 4 major aspects of tendon/ligament repair that must take place to be complete healing (8).
1st : tendon and ligament mechanical strength must be re-established. NSAID treatment has repeatedly been shown to inhibit proliferation and migration of tendon cells, but increase collagen synthesis (9-11).
NSAID treatment was shown to decrease DNA synthesis and increase protein synthesis in human tendon fibroblasts, which suggests a negative effect on tendon cell proliferation following injury but a positive effect on collagen deposition
2nd : tendons must be able to glide freely through the tendon sheath for full range of movement.
Szabo and Younger (12) have shown that NSAID treatment decreases adhesion formation and therefore increases range of motion. Four weeks of indomethacin treatment reduced adhesion formation after flexor digitorum profundus tendon transection.
There are several animal models showing reduced adhesion formation from NSAID use after injuries in multiple animal models but limited research for human models.
3rd : ligament healing must be sufficient to prevent joint laxity.
Only a single study looking at NSAIDs’ effect on joint laxity following ligament injury has been published. In this retrospective study, patients given ketorolac for 6 wks after bone-patellar tendon autograft anterior cruciate ligament reconstruction had a significant increase in anterior-posterior laxity at 6 wks post surgery when compared with non-ketorolac patients (13).
This finding suggests that NSAID therapy may increase joint laxity after a ligament injury or repair, but more research must be conducted to confirm this conclusion and determine whether the laxity is maintained, or reduces with time.
4th and finally: In those cases where the tendon or ligament insertion into the bone has been disrupted, this specialized junction (enthesis) must be reestablished with functionally equivalent mechanical strength. The enthesis progressively changes from tendon, to fibrocartilage, to calcified fibrocartilage, and finally bone.
Animal studies have shown that overall, NSAIDs appear to inhibit proper enthesis repair.
Celecoxib and indomethacin treatment of an acute supraspinatus repair in rats resulted in inconsistent regrowth of a fibrocartilage zone between the tendon and the bone, whereas control specimens showed fibrocartilage formation by 4 wk and improved collagen fiber organization by 8 wk (14)
Parecoxib and indomethacin treatment were shown to significantly lower the maximum pull-out strength and stiffness of Achilles tendons in rats that were reattached through a bone tunnel in the distal tibia (15)
Overall, NSAIDs have a some positive (preventing adhesions for tendons) but mostly negative effects on overall healing of ligaments and tendons, which is why we never recommend high doses of NSAIDs for injury recovery!
#3: What Are Some Life Threatening Dangers of Taking NSAIDs?
Heart Health:
NSAIDs can increase your risk of dying from a heart attack by > 400%!
NSAIDs can increase your risk of a second heart attack in the first 5 years after first heart attack
Here are some blogs that Dr. Centeno has highlighted the cardiac risks of various NSAIDs.
Based on our review and the advisory committees’ recommendations, the prescription NSAID labels will be revised to reflect the following information:
· The risk of heart attack or stroke can occur as early as the first weeks of using an NSAID. The risk may increase with longer use of the NSAID.
· The risk appears greater at higher doses.
· It was previously thought that all NSAIDs may have a similar risk. Newer information makes it less clear that the risk for heart attack or stroke is similar for all NSAIDs; however, this newer information is not sufficient for us to determine that the risk of any particular NSAID is definitely higher or lower than that of any other particular NSAID.
· NSAIDs can increase the risk of heart attack or stroke in patients with or without heart disease or risk factors for heart disease. A large number of studies support this finding, with varying estimates of how much the risk is increased, depending on the drugs and the doses studied.
· In general, patients with heart disease or risk factors for it have a greater likelihood of heart attack or stroke following NSAID use than patients without these risk factors because they have a higher risk at baseline.
· Patients treated with NSAIDs following a first heart attack were more likely to die in the first year after the heart attack compared to patients who were not treated with NSAIDs after their first heart attack.
· There is an increased risk of heart failure with NSAID use.
#4: NSAIDs Cause Organ Damage
Kidney Health (17)
NSAIDs reduce blood flow to your kidney
NSAIDs can cause tubular obstruction through crystal deposition (creates crystals in the tubes of your kidney blocking the flow)
Kidney stones
NSAIDs directly toxic leading to acute kidney injury (AKI).
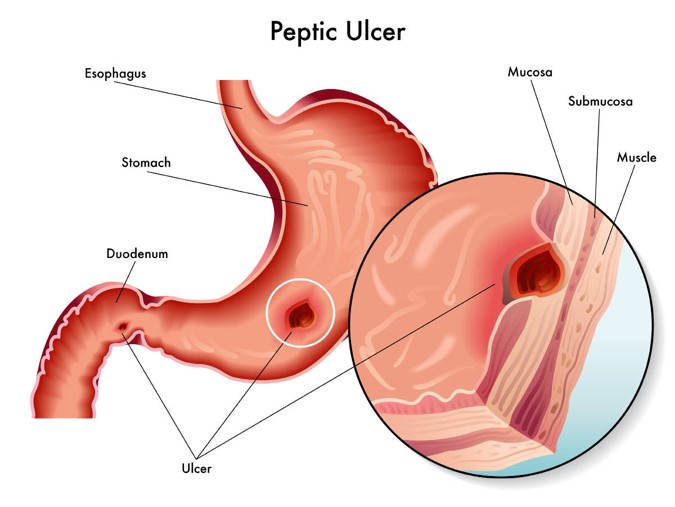
Gut Health (18)
The use of NSAIDs has been associated with the development of gastrointestinal (GI) symptoms ranging from simple dyspepsia to life-threatening GI bleeds and perforations
NSAIDs reduce the gut protection leading increased susceptibility to mucosal injury
Without mucosal protection can lead to peptic ulcers (holes in your stomach wall)
#5: Good Alternatives to NSAIDs?
Curcumin (19)
Compound derived from the dietary spice turmeric
Multiple high level studies have shown anti-inflammatory properties
Multiple research studies have placed head to head against strong NSAIDs, Curcumin has shown superiority in reduction of pain and inflammation in arthritic conditions
Recommended dosage for curcumin = 500 mg three times daily
Polyunsaturated Fatty Acids (PUFAs): Omega-3 and Omega-6 (20-22)
Omega-3 FA have been shown to be safer and more effective compared to NSAIDs for disc pain
Dose as little as 1200mg / daily was shown to be superior in pain control with less side effects!
Many additional health benefits of omega supplementation including reduction of cardiovascular disease, cancer risk, and many more
as compared to NSAIDs which increased risk for cardiovascular disease!
A lower ratio of omega-6/omega-3 fatty acids is more desirable in reducing the risk of many of the chronic diseases of high prevalence in Western societies, as well as in the developing countries, that are being exported to the rest of the world.
Excessive amounts of omega-6 polyunsaturated fatty acids (PUFA) and a very high omega-6/omega-3 ratio, as is found in today’s Western diets, promote the pathogenesis of many diseases, including cardiovascular disease, cancer, and inflammatory and autoimmune diseases
Increased levels of omega-3 PUFA (a low omega-6/omega-3 ratio) result in suppressive effects
A ratio of 4/1 was associated with a 70% decrease in total mortality. A ratio of 2.5/1 reduced rectal cell proliferation in patients with colorectal cancer, whereas a ratio of 4/1 with the same amount of omega-3 PUFA had no effect. The lower omega-6/omega-3 ratio in women with breast cancer was associated with decreased risk. A ratio of 2-3/1 suppressed inflammation in patients with rheumatoid arthritis, and a ratio of 5/1 had a beneficial effect on patients with asthma, whereas a ratio of 10/1 had adverse consequences
Bromelain (23)
A natural enzyme found in Pineapple extract has been shown to have multiple biological functions
Promotes blood flow
Speeds up wound healing
Reduces inflammation and swelling
Common dose is 400 mg twice daily
Resveratrol (24)
Sources of resveratrol in food include the skin of grapes (including red wine!), blueberries, raspberries, mulberries, and peanuts
Evidence suggests that resveratrol is a more potent anti-inflammatory agent than NSAIDs such as aspirin, ibuprofen, or indomethacin
UPSIDE:
Now that we’ve covered the top 5 things you should know about NSAIDs, there are countless reasons why NSAIDs should be avoided for acute and chronic orthopedic conditions but the good news is that there are multiple healthy alternatives to NSAIDs that should be explored and may even save your life. After educating my patient on the potential risks I highlighted above of chronic NSAID use, I was pleasantly surprised when the patient thanked me and will start weaning off their high dose of NSAIDs shortly as they start taking some of the alternatives suggested here.
Vuolteenaho K, Moilanen T, Moilanen E. Non-steroidal anti-inflammatory drugs, cyclooxygenase-2 and the bone healing process. Basic Clin Pharmacol Toxicol. 2008;102(1):10-4. Epub 2007 Oct 31.
Simon AM, Manigrasso MB, O’Connor JP. Cyclooxygenase‐2 function is essential for bone fracture healing. J Bone Miner Res 2002;17:963–76 https://www.ncbi.nlm.nih.gov/pubmed/12054171
Deguchi M, Rapoff AJ, Zdeblick TA. Posterolateral fusion for isthmic spondylolisthesis in adults: analysis of fusion rate and clinical results. J Spinal Disord 1998;11:459–64. https://www.ncbi.nlm.nih.gov/pubmed/9884288
Glassman SD, Rose SM, Dimar JR, Puno RM, Campbell MJ, Johnson JR. The effect of postoperative nonsteroidal anti‐inflammatory drug administration on spinal fusion. Spine 1998;23:834–8.
Bhattacharyya T, Levin R, Vrahas MS, Solomon DH. Nonsteroidal antiinflammatory drugs and nonunion of humeral shaft fractures. Arthritis Rheum 2005;53:364–7.
Passage and concentration-dependent effects of Indomethacin on tendon derived cells. Mallick E, Scutt N, Scutt A, Rolf C J Orthop Surg Res. 2009 Apr 2; 4():9.
Ibuprofen inhibition of tendon cell migration and down-regulation of paxillin expression. Tsai WC, Hsu CC, Chen CP, Chen MJ, Lin MS, Pang JH J Orthop Res. 2006 Mar; 24(3):551-8
Effects of celecoxib on migration, proliferation and collagen expression of tendon cells. Tsai WC, Hsu CC, Chou SW, Chung CY, Chen J, Pang JH Connect Tissue Res. 2007; 48(1):46-51.
Effects of indomethacin on adhesion formation after repair of zone II tendon lacerations in the rabbit. Szabo RM, Younger E J Hand Surg Am. 1990 May; 15(3):480-3.
The effect of ketorolac on anteroposterior knee laxity after anterior cruciate ligament reconstruction. Mehta VM, Young EP, Paxton EW, Fithian DC Orthopedics. 2008 Jun; 31(6):538-40.
Cohen DB, Kawamura S, Ehteshami JR, Rodeo SA Indomethacin and celecoxib impair rotator cuff tendon-to-bone healing. Am J Sports Med. 2006 Mar; 34(3):362-9.
Dimmen S, Nordsletten L, Engebretsen L, Steen H, Madsen JE The effect of parecoxib and indometacin on tendon-to-bone healing in a bone tunnel: an experimental study in rats. J Bone Joint Surg Br. 2009 Feb; 91(2):259-63.
Marsico F, Paolillo S, Filardi PP. NSAIDs and cardiovascular risk. J Cardiovasc Med (Hagerstown). 2017;18 Suppl 1: Special Issue on The State of the Art for the Practicing Cardiologist: The 2016 Conoscere E Curare Il Cuore (CCC) Proceedings from the CLI Foundation:e40-e43. doi: 10.2459/JCM.0000000000000443
Zhang X, Donnan PT, Bell S, Guthrie B. Non-steroidal anti-inflammatory drug induced acute kidney injury in the community dwelling general population and people with chronic kidney disease: systematic review and meta-analysis. BMC Nephrol. 2017;18(1):256 doi: 10.1186/s12882-017-0673-8.
Shep D, Khanwelkar C, Gade P, Karad S. Safety and efficacy of curcumin versus diclofenac in knee osteoarthritis: a randomized open-label parallel-arm study. Trials. 2019;20(1):214.
Maroon JC, Bost JW. Omega-3 fatty acids (fish oil) as an anti-inflammatory: an alternative to nonsteroidal anti-inflammatory drugs for discogenic pain. Surg Neurol. 2006;65(4):326-31.
Tortosa-Caparrós E, Navas-Carrillo D, Marín F, Orenes-Piñero E. Anti-inflammatory effects of omega 3 and omega 6 polyunsaturated fatty acids in cardiovascular disease and metabolic syndrome. Crit Rev Food Sci Nutr. 2017;57(16):3421-9.
Simopoulos AP. The importance of the ratio of omega-6/omega-3 essential fatty acids. Biomed Pharmacother. 2002;56(8):365-79.
Taussig SJ, Batkin S. Bromelain, the enzyme complex of pineapple (Ananas comosus) and its clinical application. An update. J Ethnopharmacol. 1988;22(2):191-203.
Oliveira ALB, Monteiro VVS, Navegantes-Lima KC, et al. Resveratrol Role in Autoimmune Disease-A Mini-Review. Nutrients. 2017;9(12):E1306.
Am I a Candidate?
To answer this question, fill out the candidate form below to request a new patient evaluation, and a patient advocate will reach out to you to determine your next steps. Your one-hour, in-office or telemedicine evaluation will be with one of the world’s experts in the field of Interventional Orthopedics.