It started as a nuisance and has now has progressed. Shoulder pain radiating down arm to fingers is now constant. Rest and NSAIDs are not effective. What is Cervical Radiculopathy? What is the basic anatomy of the neck? What causes cervical radiculopathy? What are the symptoms of Cervical Radiculopathy? How is Cervical Radiculopathy diagnosed? What are the treatment options? What are the regenerative treatment options? Meet GB. Let’s dig in.
What Is Cervical Radiculopathy? (AKA Pinched Nerve)
Cervical Radiculopathy is a clinical condition in which a nerve or nerves in your neck become irritated or compressed. It is also known as ” a pinched nerve“. The causes are discussed below. It can affect individuals of any age with peak prominence between ages 40-50 years of age (1).
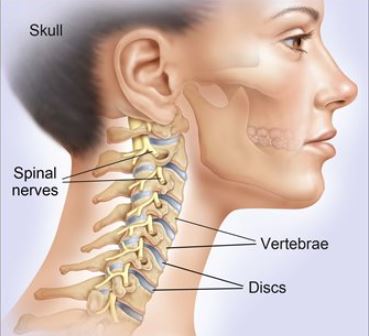
Basic Anatomy of the Neck (Bones, Discs & Nerves)
Bones
There are 7 boney building blocks that make up your spine. They are called vertebral bodies. They are numbered from 1 to 7 and preceded by the letter C to denote Cervical. For example, the first bone in the cervical spine is the C1.
Discs
Sandwiched between each of the neck bones is a soft, compressive wafer also known as a disc. The disc is very important as it absorbs and distributes the forces of daily living. It is made up of two components.
Annulus Fibrous
This refers to a thick tough outer layer that surrounds the disc. It is similar to the sidewall in a tire. It encases and protects the gel-like center.
Nucleus Pulposus
Gel-like material in the center of the disc. It is composed of water, collagen, and proteoglycans (2). The Nucleus Pulposus stability and flexibility for the spine.
The discs are susceptible to injury. Common examples include disc bulges, disc herniations, and extrusions.
Nerves
Nerves exit the spinal cord as it travels down into the spine. At each level of the spine a specific nerve exits. For example, at the C5/6 level, the C6 nerve exits the spine. It provides important information to that part of the body. The nerve exits through a boney doorway just as you exit your home or office daily. This doorway is also known as the Neural Foramen. It is composed of bone. Nerves are very fragile and are surrounded by fat which provides protection and a level of cushion. The Neural Foramen can be narrowed which can cause irritation, compression, or injury to the exiting nerve. Causes and symptoms are discussed below.
What Causes Cervical Radiculpathy?
Cervical Radiculopathy is due to spinal nerve inflammation, irritation, or compression. The most common causes of Cervical Radiculopathy are:
Disc Injury
The disc is an important shock absorber. Unfortunately, it is susceptible to injury. Examples include disc bulges, herniations, and extrusions. These injuries can irritate or compress the exiting nerve root. This results in a “pinched nerve”. Disc herniation accounts for approximately 21.9% of Cervical Radiculopathy cases (3).
Cervical Spine Degeneration
Degeneration of the cervical spine can result in a narrowing of the bony doorway through which the spinal nerve exits. Irritation or compression of the nerve can result in pain radiating down the arm to the fingers.
Tumor
A tumor whether malignant or benign may grow near the Neural Foramen and push against the nerve root.
Trauma
Weekend warrior endeavors, repetitive motion activities, and motor vehicle accidents can cause irritation of the spinal nerve with pain and dysfunction.
Facet Joint Overgrowth
A facet is a small paired joint on the backside of the spine. It provides important stability and limits movement. There is a facet joints at each level of the spine. Trauma, inflammation, and degeneration can cause the joint to become injured and enlarged. Overgrowth of the facet joint can cause narrowing of the Neural Foramen with subsequent irritation or compression of the exiting nerve.
Synovial Cysts
The facet joint is lined with cartilage and covered with a protective membrane called the synovium. A Synovial Cyst is a fluid-filled sac that can develop in the facet joint. The Synovial Cyst can create pressure and irritation or compression of the exiting nerve. Ouch!
L5-S1 Annular Tear
The labrum is a cartilaginous cup that circles the shallow shoulder socket (the glenoid) to make the socket deeper. The labrum supports and stabilizes the shoulder joint. Causes of Shoulder Labral Tears
Injury to the labrum typically occurs from repetitive trauma in overhead throwers, such as in baseball. It can also occur from a traction injury to the arm, such as lifting a heavy object off the ground or getting your arm jerked. Symptoms of Shoulder Labral Tears. Typical symptoms include pain in the front of the shoulder or deep inside the joint. Treatment options initially include physical therapy which is designed to restore range of motion and strength to the shoulder.
AC joint Impingement is a painful condition that occurs when the space beneath the acromion bone is narrowed. This narrowing can result in irritation of the rotator cuff tendons and bursa. A bursa is a fluid-filled sac that reduces the friction on tendons and muscles as they cross bony surfaces. A tendon is thick collagen tissue that connects muscles to bones. The rotator cuff tendons provide important support and enable movement in the shoulder. If severe, impingement can cause tears in the rotator cuff tendons. Patients with AC joint impingement typically have pain with elevation of the arm and or while lying on the shoulder.
Avascular Necrosis is essentially a lack of blood flow, eventually resulting in necrosis, or dying of the bone. This happens in multiple joints. And today we are talking specifically about the shoulder. So talking about AVN in the shoulder, patients typically come up with two main questions. Number one, can this heal on its own? And if not, how long or how fast will this progress? Now we classify AVN in multiple different stages: Number one: we have stage one, where it is very normal X-ray — usually, typically, someone just has pain with activity. Is the bone itself continues to deteriorate, then we start getting some changes on your X-ray.
Calcific tendonitis of the rotator cuff is a relatively common yet frequently misunderstood shoulder condition. Characterized by the deposition of calcium crystals within the tendons of the rotator cuff, this ailment can lead to significant pain and limited mobility for the affected individual. While it often strikes seemingly out of the blue, its origins and progression are rooted in a combination of biological processes, genetics, and, potentially, lifestyle factors. This article aims to delve deep into the intricacies of this condition, shedding light on its causes, symptoms, treatment options, and preventive measures. This article aims to delve deep into the…
Disorders that affect and weaken the connective tissues such as tendons and ligaments. It is a hereditary disorder which means you are born with it. EDS has many different signs and symptoms which can vary significantly depending upon the type of EDS and its severity. It most commonly affects the skin, joints, and blood vessels. Joints are typically hypermobile with excessive joint range of motion because of a defect in collagen formation. In most cases Ehlers-Danlos syndrome is inherited. That is to say that you are born with it. The two main ways EDS is inherited are: autosomal dominant inheritance and autosomal recessive inheritance…
Frozen shoulder, also known as adhesive capsulitis, is a painful loss of shoulder movement and range in motion. The incidence of frozen shoulder is 3-5% in the general population and up to 20% in those with diabetes. The peak incidence is between 40-60 years of age. The exact mechanism is poorly understood. In general, the capsule becomes inflamed, thickened, and contracted with pain and significant restriction in range of motion. causes are poorly understood but risk factors include trauma, prolonged immobility, systematic diseases such as diabetes, stroke, connective tissue disease, and heart disease. Other causes include post-surgery, chronic inflammation causing stimulation of myofibroblasts
Are you plagued by shoulder pain that has now transitioned from intermittent to constant and keeps you up at night? Are daily shoulder movements, such as dressing and reaching for objects in the kitchen cabinets, painful? Is your range of motion decreasing as your pain is increasing? You may have a full- or partial-thickness rotator cuff tear. Has conservative therapy in the form of heat, ice, stretching, rest, and acupuncture failed to provide significant relief? Has an MRI demonstrated a full-thickness or partial-thickness tear of the rotator cuff? What to do? If left untreated, full-thickness and 26% of partial-thickness tears will progress.
Arthritis in the shoulder can present with different symptoms based on the underlying cause of the arthritis. Here’s a list of symptoms associated with shoulder arthritis: Pain can occur in different shoulder locations, which can indicate which part is affected: When the acromioclavicular (AC) joint is affected, the pain is usually experienced at the top of the shoulder. Pain surrounding the shoulder can indicate an involvement of the rotator cuff. The pain can disrupt joint
Pain is the most common symptom. It typically occurs with the elevation of the arm, forced movement overhead, and when lying on the shoulder. Impingement can also cause shoulder pain when reaching across the body. Narrowing of the subacromial space is the most common cause of shoulder impingement syndrome (6). The subacromial space is the area between the top of the arm bone (humerus) and the AC joint. This narrowing compresses or pinches the rotator cuff tendons and bursa. If left untreated the rotator cuff tendons can become inflamed, damaged, and or torn.Bursa and tendons can not be seen on x-ray. An x-ray may demonstrate…
The labrum is a cartilaginous cup that circles the shallow shoulder socket (the glenoid) to make the socket deeper. The labrum supports and stabilizes the shoulder joint. Causes of Shoulder Labral Tears
Injury to the labrum typically occurs from repetitive trauma in overhead throwers, such as in baseball. It can also occur from a traction injury to the arm, such as lifting a heavy object off the ground or getting your arm jerked. Symptoms of Shoulder Labral Tears. Typical symptoms include pain in the front of the shoulder or deep inside the joint. Treatment options initially include physical therapy which is designed to restore range of motion and strength to the shoulder.
On average, a swimmer swims 60,000 meters per week. A large proportion of the forward propulsion in swimming is generated by the upper body. 90% of the driving force in the upper body comes from the torque generated by the shoulder. As a result, the shoulder is put under tremendous load during various swimming strokes to generate this propulsive force. Similar forces act on the shoulder when a person lifts heavy weights overhead or works in a profession or sport with the same shoulder movement. These forces can lead to swimmer’s shoulder, whether caused by impingement of a nerve, a tear in the…
The thoracic outlet is an area around the collar bone where the nerves that come from your neck meet up with the blood vessels from your heart and together supply the entire upper extremity (shoulder and arm). These blood vessels (subclavian artery and vein) and nerves (brachial plexus) travel from the base of your neck to your armpit (axilla) and are considered the “thoracic outlet”. Now that you know what the thoracic outlet is, what is thoracic outlet syndrome? Simply listening to a patient’s history and completing a physical examination is all that is needed to diagnose TOS. But more involved imaging such as X-rays…
Thoracic Spine Tumor: Symptoms, Causes, and Treatment Options
The labrum is a cartilaginous cup that circles the shallow shoulder socket (the glenoid) to make the socket deeper. The labrum supports and stabilizes the shoulder joint. Causes of Shoulder Labral Tears
Injury to the labrum typically occurs from repetitive trauma in overhead throwers, such as in baseball. It can also occur from a traction injury to the arm, such as lifting a heavy object off the ground or getting your arm jerked. Symptoms of Shoulder Labral Tears. Typical symptoms include pain in the front of the shoulder or deep inside the joint. Treatment options initially include physical therapy which is designed to restore range of motion and strength to the shoulder.
The temporomandibular joint (TMJ) is the joint connection between your jaw and your skull. If you run your fingers along either side of your jaw line toward your ears, you can actually feel where the jaw bone ends and the skull bone begins. If you open and close your mouth, the difference between the two is dramatic as the jaw bone moves, thanks to the TMJ joint, while the skull bone remains stable. The TMJ and any of its surrounding structures can become painful and inflamed, and this can become so bad that it can prevent patients from even being able to move their jaw bone to chew.
Symptoms vary depending upon the severity and location of the injury. They may be limited to one side or conversely can affect both sides of the neck and arms. The most common symptoms include
Determining the cause of cervical radiculopathy begins with a complete history of physical examination. Details of previous traumas including motor vehicle accidents are important. At the Centeno-Schultz Clinic, you will spend quality time with a board-certified, fellowship-trained physician who is committed to your care and success. Specific physical examination tests will be performed to document weakness, numbness, and neck function. This may include:
How well you can bend your neck and roll your head in all directions
If there is tenderness around the neck
If there are muscle spasms around the neck and shoulders
Areas of tenderness that create shooting pain down shoulder or arm
Radiographic studies are necessary and include:
X-ray: Useful to document narrowing of disc spaces, Neural Foramen narrowing and curvature of the spine (Scoliosis)
CT AKA CAT Scan: Helpful to access bone spurs, narrowing of the Neural Foramen, facet overgrowth and calcifications of the spinal ligaments. Diagnostic accuracy is between 72-81% (4).
MRI: The most common imaging for Cervical Radiculopathy with a diagnostic accuracy of 88% (5). MRI captures muscles, ligaments, tendons, nerves, and all boney structures along with any narrowing of the neural foramen.
Cervical Radiculopathy Treatment Options?
Treatment options will depend upon the severity of the injury and clinical symptoms. When appropriate conservative care should always be the first line of therapy.
Conservative Care
Options include rest, safe anti-inflammatory medications, chiropractic care, and physical therapy. Gentle cervical traction, mobilization, and strengthening are oftentimes helpful. To treat the burning arm pain some patients are starting on nerve medications like Neurontin, Lyrica, or Cymbalta. The nerve pain is rarely responsive to oral narcotics.
Steroids
Steroids are powerful anti-inflammatory medications. They can be taken orally, injected into the muscle, or injected into the spine. Examples of commonly used steroids include Depo-Medrol, Betamethasone, dexamethasone, triamcinolone, Celestone, and Kenalog. The dangerous side effects have been discussed in previous blogs. The major side effects include:
Destroying cartilage (6)
Increasing the risk of infection
Systematic Problems
Surgical Treatment
Surgery is often recommended when conservative care and steroids fail to provide signficant or sustained benefit. The specific type of surgery will depend upon the cause and severity of the injury. Discectomy is a common surgical procedure where the protruding disc is surgically trimmed in a hope of reducing the pressure and irritation on the spinal nerve. Unfortunately trimming of the disc can further weaken the disc side wall predisposing the disc to future injury including herniation and disc degeneration.
Regenerative Treatment Options
At the Centeno-Schultz Clinic we are experts in the treatment of neck injuries. We stopped using high dose steroids and nerve burning procedures in 2005. Treatment options include precise x-ray guided injections of PRP and Bone Marrow Concentrate which contains stem cells. All procedures are performed by board certified, fellowship trained physicians under x-ray or ultrasound guidance. Treatment goals are to reduce inflammation and improve blood flow for best clinical outcomes. Our clinical results are available here.
To better understand what occurs with a disc injury and why steroids and surgery are not your best option please click on the video below.
Meet GB
GB is a 49 y/p competitive tennis player who was referred by his chiropractor. He had a several-month history of right arm numbness and weakness that was constant and unresponsive to conservative or chiropractic care. The onset of symptoms was not associated with any trauma. The forearm weakness and tingling in his fingers were progressive in nature. He specifically denied any neck pain, tension or restriction in range of motion. Physical examination was most significant for right arm weakness, diminished sensation to light touch and pain in his mid to lower neck aggravated by rotation and looking upward. MRI of the cervical spine was notable for 2 level disc injury with severe compression of the exiting spinal nerves.
GB underwent x-ray guided PRP injections into areas of injury. This included a two-level epidural injection, facet injection, and supporting ligaments. The procedure was performed at the Centeno-Schultz Clinic in Broomfield, Colorado. An ambulatory surgical center or hospital suite was not required as we have several state-of-the-art procedure rooms within the clinic.
Here are his self-reported results.
1 month after treatment GB noted significant improvement.
“Thirty days later and I can say that I am a believer in your work. I have not gotten onto a tennis court since before the PRP injection, but I can tell you that the numbness in my ring finger is completely gone and my pinkie finger is 95% back. The numbness in the back of my hand is totally gone and (probably most importantly) I feel like the strength in my forearm has returned. I no longer struggle with the simple tasks I did prior to the procedure (doing the dishes, tying my shoes, brushing my teeth, lifting my laptop…)”.
At 9 months following the treatment GB continued to improve.
“We are now nearly 38 weeks past the day of the procedure. I can tell you that whatever Dr. Schultz did inside my neck completely cured the problem. While I did have to rebuild strength and regain some of my form on the tennis court, to this day I have no numbness in my hand, and my arm is back to full strength. For what it’s worth, in May my doubles partner and I won a National level tournament title in our age division (50’s) in Boise and I’ve successfully captured singles victories in Scottsdale as well as here in Denver.
Thank you for the work performed on my neck; allowing me to regain the ability to play tennis at a high level. I am thrilled at the results of the PRP procedure.”
In Conclusion
Cervical Radiculopathy is a medical condition in which a nerve or nerves in your neck become irritated or compressed. Also kinown as ” A Pinched Nerve”.
The cervical spine is made up of bones, discs, and nerves
Cervical Radiculopathy is due to spinal nerve inflammation, irritation, or compression. The major causes include disc injury, disc degeneration, tumor, trauma, or facet overgrowth.
Common Cervical Radiculopathy symptoms include neck pain, arm pain, shoulder pain radiating down arm to fingers, numbness, tingling, and weakness
Diagnosis requires history, physical examination, and in most cases radiographic studies. MRI is the preferred study of choice.
Treatment options include conservative care, steroids, and steroids.
PRP and Bone Marrow Concentrate injections allow patients to avoid the significant complications of steroids and surgery.
If you’re suffering from symptoms associated with shoulder pain radiating down arm to fingers, numbness, tingling, or arm weakness, please make sure to consider Regenexx procedures for cervical conditions at Centeno-Schultz Clinic. You can schedule an evaluation in office or from the comfort of your home. Make the first move to recover from your injury or condition today!