Shoulder Cracking
Get Help With Shoulder CrackingShoulder crackling, popping, and grinding can be painful. Unfortunately these symptoms often times get a blank stare from physicians. What is the Scapula? What is Snapping Scapula? What causes a Snapping Scapula? How do you fix a Snapping Scapula? Are there regenerative options? Let’s dig in.
What is the Scapula?
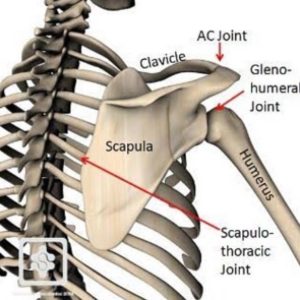
The Scapula is your shoulder blade. It is a large triangular bone that compromises part of the shoulder joint. The Scapula is positioned over the back chest wall and ribs where it moves in different directions with shoulder movements (1). The Scapula meets with the arm bone (humerus) to form the shoulder joint. It also meets with the clavicle to form the AC joint. Multiple structures attach onto the Scapula which provides important support and movement for the scapulae and shoulder joint (2). These include:
Muscles/Tendons: Multiple muscles attach to the Scapula which include the deltoid, supraspinatus, infraspinatus, triceps, and teres minor. These muscles work together to coordinate a smooth sliding of the scapula on the chest wall.
Ligaments: Multiple ligaments attach to the Scapula providing important support and movement of the scapula. Ligaments are thick bands of connective tissue that connect one bone to another. Major ligaments include the superior, inferior glenohumeral and coracohumeral ligaments.
Bursae: Fluid sacs that facilitate the movement of tendons, ligaments, and muscle over the boney Scapular surface. The scapulothoracic and subscapularis bursa and the two most commonly involved bursae.
What Is Shoulder Crackling?
Snapping Scapula is a medical condition that involves the audible popping and grinding of the Scapula over the rib cage during shoulder movements. It is also referred to as washboard syndrome. It typically affects young, active patients (3). Many describe audible popping and crackling with shoulder movement (4). Common symptoms include:
- Shoulder tenderness with restriction of movement
- Grinding, grating and snapping sensation
- Swelling
- Pain during overhead activities (5)
What Causes Shoulder Crackling?
The are many causes of snapping Scapula which include:
Muscle injury or Imbalance: Scapular movement requires a coordinated balance between muscles and tendons. When muscles weaken or tendons become inflamed, muscle imbalance can occur. When this occurs the Scapula can not easily glide along the chest wall. The result can be grinding and snapping of the scapula.
Bursae Inflammation: the most commonly involved are the scapulothoracic and subscapularis bursae (6).
Irritation of Neck Nerves: disc bulges, disc herniation, facet overgrowth and slipped discs can irritate or compress nerves. This in turn can cause muscle weakness and scapular muscle imbalance and snapping.
Repetitive activities such as reaching overhead or throwing a ball.
Poor posture that compromises neutral spinal alignment.
Inflammatory Conditions such a rheumatoid arthritis
Bone Tumors: the most common is an osteochondroma which due to its mass effect can create a scapular winging along with popping and grinding (7)
Trauma: Fractures of the rib or Scapula can compromise the smooth gliding of the Scapula on the rib cage leading the grinding, snapping, and oftentimes pain.
Nerve injury: Injury or compression of the long thoracic nerve, dorsal scapular nerve, and spinal accessory nerve can create muscle imbalance leading to grinding and popping of the Scapula.
Shoulder Tendonitis
A tendon is a thick connective tissue connecting muscle to bone. It functions to transmit the force generated by the muscle contractions to the bones, enabling movement of the associated joint. The rotator cuff and the biceps tendon are the major tendons in the shoulder. The rotator cuff is composed of four major tendons: supraspinatus, infraspinatus, subscapularis, and teres minor. The rotator cuff tendons provide shoulder stability and facilitate arm movement and are therefore
Read More About Shoulder TendonitisAvascular Necrosis of the Shoulder
Avascular Necrosis is essentially a lack of blood flow, eventually resulting in necrosis, or dying of the bone. This happens in multiple joints. And today we are talking specifically about the shoulder. So talking about AVN in the shoulder, patients typically come up with two main questions. Number one, can this heal on its own? And if not, how long or how fast will this progress? Now we classify AVN in multiple different stages: Number one: we have stage one, where it is very normal X-ray — usually, typically, someone just has pain with activity. Is the bone itself continues to deteriorate, then we start getting some changes on your X-ray.
Read More About Avascular Necrosis of the ShoulderEhlers-Danlos Syndrome (EDS)
Disorders that affect and weaken the connective tissues such as tendons and ligaments. It is a hereditary disorder which means you are born with it. EDS has many different signs and symptoms which can vary significantly depending upon the type of EDS and its severity. It most commonly affects the skin, joints, and blood vessels. Joints are typically hypermobile with excessive joint range of motion because of a defect in collagen formation. In most cases Ehlers-Danlos syndrome is inherited. That is to say that you are born with it. The two main ways EDS is inherited are: autosomal dominant inheritance and autosomal recessive inheritance…
Read More About Ehlers-Danlos Syndrome (EDS)Frozen Shoulder
Frozen shoulder, also known as adhesive capsulitis, is a painful loss of shoulder movement and range in motion. The incidence of frozen shoulder is 3-5% in the general population and up to 20% in those with diabetes. The peak incidence is between 40-60 years of age. The exact mechanism is poorly understood. In general, the capsule becomes inflamed, thickened, and contracted with pain and significant restriction in range of motion. causes are poorly understood but risk factors include trauma, prolonged immobility, systematic diseases such as diabetes, stroke, connective tissue disease, and heart disease. Other causes include post-surgery, chronic inflammation causing stimulation of myofibroblasts
Read More About Frozen ShoulderShoulder Arthritis
Arthritis in the shoulder can present with different symptoms based on the underlying cause of the arthritis. Here’s a list of symptoms associated with shoulder arthritis: Pain can occur in different shoulder locations, which can indicate which part is affected: When the acromioclavicular (AC) joint is affected, the pain is usually experienced at the top of the shoulder. Pain surrounding the shoulder can indicate an involvement of the rotator cuff. The pain can disrupt joint
Read More About Shoulder ArthritisShoulder Impingement Syndrome
Pain is the most common symptom. It typically occurs with the elevation of the arm, forced movement overhead, and when lying on the shoulder. Impingement can also cause shoulder pain when reaching across the body. Narrowing of the subacromial space is the most common cause of shoulder impingement syndrome (6). The subacromial space is the area between the top of the arm bone (humerus) and the AC joint. This narrowing compresses or pinches the rotator cuff tendons and bursa. If left untreated the rotator cuff tendons can become inflamed, damaged, and or torn.Bursa and tendons can not be seen on x-ray. An x-ray may demonstrate…
Read More About Shoulder Impingement SyndromeHow Do You Fix a Shoulder Crackling?
Treatment options depend upon the underlying cause of the shoulder crackling. In general conservative treatment is the first-line treatment. It includes rest, safe anti-inflammatory medications, and PT. PT focuses on muscle dysfunction, compromised posture, and improper shoulder joint mechanics (8). When conservative therapy fails, steroid injections are often recommended. (9). Steroids are powerful anti-inflammatory agents that deplete local stem cells and are toxic to cartilage and weakens tendons and ligaments (10). If pain persists despite injections and conservative care, surgery is many times recommended. There are two major surgeries.:
- Surgical removal of an inflamed bursa and surrounding scar tissue
- Partial removal of the Scapula to reduce areas that are rubbing on the rib cage. Unfortunately, important muscles, tendons, and ligaments attach to the scapula. Surgery can lead to changes in the biomechanics of the shoulder and create instability.
Is there a regenerative option? YES
SANS
At the Centeno-Schultz Clinic, we are experts in shoulders, tendons, and ligaments. We utilize a comprehensive approach to a given joint, It stands for
- Stability,
- Articulation,
- Neurologic, and
- Symmetry.
Using ultrasound we can evaluate the ligaments, tendons, muscles nerves, and bursa of the shoulder. Ultrasound can identity ligament laxity, nerve compression, and tendon tears. Treatment options include PRP and stem cells. PRP is rich in growth factors that can increase blood flow and decrease inflammation. The injections are demanding and can not be performed by your PCP or orthopedic surgeon. To learn more about stem cell and PRP injections into the shoulder please click on the video below.
In Conclusion
The Scapula is your shoulder blade. It is a large triangular bone that resides on the back chest wall and ribs and moves in different directions with shoulder movements. Muscles, tendons, ligaments, and bursa attach to the Scapula providing important support.
Snapping scapula is a medical condition that involves audible popping and grinding over the rib cage during shoulder movements. Symptoms include shoulder tenderness, swelling, and pain during overhead activities. Causes of snapping scapula include muscle injury and imbalance, inflamed bursa, irritation of neck nerves, poor posture, inflammatory conditions, bone tumors, trauma, and nerve injury. Conservative care is the first line of treatment.
Steroid injections are powerful anti-inflammatory agents that deplete local stem cells and are toxic to cartilage, tendons, and ligaments and therefore should be avoided. Surgery is recommended if pain persists despite conservative care and injections. Surgery focus on the removal of an inflamed bursa or a portion of the boney Scapula which can compromise the stability of the shoulder.
A novel technique at the Centeno-Schultz Clinic utilizes the SANS approach where the stability, articulation, symmetry, and neurologic components are assessed. Ultrasound is a powerful technology that allows muscles, tendons, ligaments, and bursa to be visualized during an in-office evaluation. This approach is superior to toxic steroids and surgery which can permanently change the mechanics of the Scapula and the stability of the shoulder. If you are limited by Snapping Scapula please schedule a Telemedicine evaluation where board-certified, fellowship-trained physicians can review your history, imaging and discuss non-surgical treatment options for shoulder pain. Don’t be sidelined by scapular pain as natural, nonsurgical options exist.
1.Paine R, Voight ML. The role of the scapula. Int J Sports Phys Ther. 2013;8(5):617-29.
2.Kamkar A, Irrgang JJ, Whitney SL. Nonoperative management of secondary shoulder impingement syndrome. J Orthop Sports Phys Ther. 1993;17:212–224
3.de Carvalho SC, Castro ADAE, Rodrigues JC, Cerqueira WS, Santos DDCB, Rosemberg LA. Snapping scapula syndrome: pictorial essay. Radiol Bras. 2019;52(4):262-7.
4.Kouvalchouk JF. Subscapular crepitus. Orthop Trans. 1985;9:587–588
5.Kuhn JE, Plancher KD, Hawkins RJ. Symptomatic scapulothoracic crepitus and bursitis. J Am Acad Orthop Surg. 1998;6:267–273.
6. Snapping scapula syndrome. Lazar MA, Kwon YW, Rokito AS J Bone Joint Surg Am. 2009 Sep; 91(9):2251-62.
7..Delayed Presentation of Osteochondroma at Superior Angle of Scapula-A Case Report.Jindal M. J Orthop Case Rep. 2016 Jul-Aug; 6(3):32-34.
8. Manske RC, Reiman MP. Nonoperative and operative management of snapping scapula. Am J Sports Med. 2004;32:1554–1565.
9.Symptomatic scapulothoracic crepitus and bursitis. Kuhn JE, Plancher KD, Hawkins RJ J Am Acad Orthop Surg. 1998 Sep-Oct; 6(5):267-73.
10.Wernecke C, Braun HJ, Dragoo JL. The Effect of Intra-articular Corticosteroids on Articular Cartilage: A Systematic Review. Orthop J Sports Med. 2015;3(5):2325967115581163.