Elbow pain can be agonizing, making simple movements of your arm almost impossible. Two common causes of elbow pain are tennis elbow and golfer’s elbow. People often confuse the two and often wonder how they can develop this condition when they have never played tennis or golf.
That’s exactly what this post will discuss. How do you develop tennis elbow or golfer’s elbow? What is the difference between a golfer’s elbow and a tennis elbow? Can someone have both of them at the same time? How do you treat them? What is the best treatment? Let’s dig in.
The Elbow Anatomy
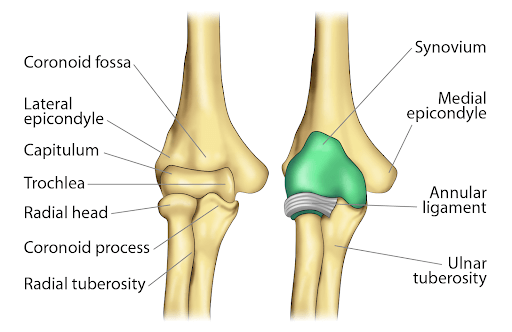
The elbow joint is largely a hinge joint that also has the unique ability to rotate. It is composed of three principal bones: the upper arm bone (humerus) and the two bones that make up the forearm, the radius, and ulna. There are two important bony surfaces on the humerus that are called epicondyles.
The medial epicondyle is on the inside of the elbow joint, whereas the lateral epicondyle is on the outside. The epicondyle is where tendons and ligaments attach. Tendons are thick bands of connective tissue that connect muscle to bone, whereas ligaments connect bone to bone and act like pieces of duct tape to provide stability to a joint.
The lateral epicondyle is where the extensor and supinator tendons and collateral ligaments attach. The medial epicondyle is where the flexor and pronator tendons and collateral ligaments attach. Because tendons have poor blood supply compared to muscle tissue, they are susceptible to injury including inflammation, tears, and ruptures.
Repetitive motions like flexion and extension with force and sports injuries can cause small tears to the tendons attached to the medial and lateral epicondyles giving rise to golfer’s elbow and tennis elbow.

Golfer’s Elbow And Tennis Elbow: Know The Difference
Both conditions involve inflammation, micro injury and degeneration of the tendons at their attachment to the epicondyle, which is also called epicondylitis or tendinosis. The difference is in the location. Tennis Elbow, also known as lateral epicondylitis or common extensor tendinosis, is inflammation and injury and pain on the outside of the elbow.
Golfer’s elbow, which is also known as medial epicondylitis or common flexor tendinosis, affects the inside of the elbow. If it helps, Tennis, Lateral and outside all have T‘s, so it’s an easy way to remember that Tennis elbow involves the LaTeral or OuTside of the elbow. Pain with movement is the primary symptom.
Tennis Elbow (Lateral Epicondylitis)
Lateral epicondylitis occurs in approximately 1-3% of the population annually and is most common in 30-50-year-olds (2). Symptoms typically occur due to overuse or strain from repetitive gripping or wrist extension. Risk factors for lateral epicondylitis are increased age, increased BMI, rotator cuff disease, carpal tunnel syndrome, oral steroid use, and smoking (3).
Golfer’s Elbow (Medial Epicondylitis)
This condition is less common than lateral epicondylitis with a prevalence of less than 1% (4). Patients at risk include overhead throwers and workers lifting heavy objects (5).
Other important causes of pain on the inside of the elbow include ulnar nerve disorders, nerve irritation in the cervical spine, and laxity or tearing of the ulnar collateral ligament complex (6). Pain is typically gradual in onset and may be accompanied by grip strength weakness (7).
Is It Possible To Have Tennis Elbow And Golfer’s Elbow At The Same Time?
Yes, it is possible to have tennis elbow and golfer’s elbow at the same time regardless of whether you play sports or not. While golfer’s elbow is less common than tennis elbow, you can have both conditions simultaneously that present with generalized elbow pain.
Construction workers, rock climbers, and plumbers who perform multiple forearm movements with high tensile strength and torque (rotational movement) for a long time can develop these conditions.
Sports-Related Causes
There are various sports that cause athletes to develop tennis elbow and golfer’s elbow. They include the following:
- Weight Training: Weight training involves lifting heavy weights repeatedly. This repetitive motion with heavy weights can strain the medial and lateral epicondyle. These motions can inflame the tendons attached here giving rise to elbow pain.
This can develop faster if an individual doesn’t pace himself with the weights and tries to lift too much too fast before letting the muscles develop gradually.
- Football: In football, repetitive overhead throwing movements or even poor throwing technique can cause inflammation, tears, and ruptures of the tendons attached at the condyles. This occurs especially when players attempt to throw further away and end up straining the joint by using more force.
- Archery: In archery, athletes’ elbows are under a lot of stress especially when they bring the bow to a full draw. As the athlete pulls back the string the bowstring elbow flexes and the medial muscles have to do more work. This causes micro tears in the medial muscles and tendons. And so sometimes tennis elbow is also called archer’s elbow.
There’s also the fact that there is a significant amount of hand shock that is transmitted from the bow into the elbow as it is released.
- Javelin throwing: Javelin throwers develop tennis elbow mainly due to overuse/ This occurs when they subject the ulnar collateral ligament to a very high force that displaces the joint away from the midline of the body. Since the ulnar collateral ligament opposes this motion, over time it develops tears. It may also be known as javelin thrower’s elbow.
Causes Not Related To Sports
Various activities that involve repetitive motions similar to golfers and tennis players also develop tennis elbow and golfer’s elbow. They include:
- Carrying heavy luggage: For people who carry heavy luggage or material like porters, baggage handlers, and manual handlers in post or cargo work, their work strains the ligaments of the elbow.
The motion is similar to that of golfers and tennis players but with far more weight attached which causes tears and ruptures in the elbow ligaments and tendons giving rise to tennis and golfers’ elbow.
- Overhead movement: In construction workers and painters, there is plenty of overhead movement of the elbow. Construction workers have to throw heavy overhead material that can strain the tendons as well as try to generate significant force to have the item reach a designated height or location.
- Frequent use of hand tools and power machinery: A butcher cutting meat, a weaver, a crocheter, plumbers, and mechanics who use screwdrivers and hammers are all susceptible to elbow pain due to tennis elbow and golfers elbow because of the repetitive motion.
The repeated movements can shear the tendons and ligaments at a microscopic level which does not heal since these motions occur multiple times during a day. And so even though there’s not much torque or weight involved with these activities, just the overuse of these tendons and muscles of the elbow can cause these conditions.
Home Treatment Options For Medial Epicondylitis
Golfer’s elbow can be treated with home remedies that are simple and can be done easily. They include the following:
- Ice pack application: Applying ice packs can reduce the inflammation in the area as they can constrict the blood vessels and reduce blood flow. This can only be done for ten-minute intervals when the pain is severe. Frequent usage of ice is not particularly recommended as ice limits blood flow and can impede healing.
- Forearm brace: A forearm brace can be a strap or an orthosis that is worn over the forearm and puts direct pressure on the forearm tendons. It also absorbs extra forces transmitted through the muscles during activity. It can change the angle at which the tendon works thus allowing the injured areas to heal.
- Night splint: The night splint is a splint that is worn over the elbow all night and prevents it from bending or flexing. The splint allows some movement but generally keeps the elbow immobilized which allows the microtears and injured areas to recover.
- Strengthening exercises: Once the pain is less, strengthening exercises for the elbow is important to build stronger muscles. This will treat the pain and prevent future elbow injuries. These are eccentric exercises such as the fist clench exercise, supination exercise with a light weight, and towel twist exercise.
Professional Interventions For Golfer’s Elbow And Tennis Elbow
Treatment options depend upon the severity of the injury, past medical history, access to medical care, and your physician’s preferences. It is always best to start with conservative therapy. Conservative therapy includes physical therapy, injections, and pain management. If symptoms do not improve with conservative management then surgery is another option.
Physical Therapy And Traditional Treatments
Traditional treatment includes activity modification, physical therapy, and acupuncture. Research has shown that therapeutic tape also helps improve both grip strength and pain (1).
Physical therapy involves both strengthening and stretching exercises. These are not just aimed at the elbow but the wrist as well. The exercises focus on stretching and strengthening the muscles of the forearm.
Steroids
Corticosteroids are powerful anti-inflammatory agents that can provide short-term benefits in pain relief. These injections are used to reduce inflammation when the pain is severe. It is usually given along with a local anesthetic like lidocaine.
Unfortunately, they can also cause cell death, skin atrophy, compromise immune system function and repair, and must be used with caution (9). These are typically not recommended by our clinic in the traditional high milligram doses.
NSAIDS
NSAIDs (Nonsteroidal anti-inflammatory drugs) are often recommended for pain management. NSAIDs should not be used long-term due to their effect on the kidney and the gastric lining (8).
They can relieve inflammation and reduce pain in the short term but are not a permanent treatment for golfers’ elbow and tennis elbow. More recent data has shown that chronic use can accelerate joint degradation and worsen arthritis.
Surgery
Many surgical options exist depending on the severity of the injury, including stripping away a portion of the tendon sheath to promote healing. The goal is to clean out any dead tissue and repair any tendon tears.
Graft procedures can also be used with autografts from the individual’s body can be used as the palmaris longus, gracilis, semitendinosus, toe extensor, plantaris, patellar tendon, or Achilles autograft.
Surgery may also involve the nerves, especially with medial epicondylitis, where the ulnar nerve is often decompressed or repositioned (10). Complications can occur and include loss of grip strength (11). Also, infection, escalation of pain, ligament instability, neuroma formation, and late return to work because of prolonged postoperative recovery time can occur (12).
What Is The Best Non-Surgical Alternative?
The best non-surgical alternative for the treatment of medial epicondylitis is platelet-rich plasma (PRP). PRP injections have been more effective than steroids for this condition(13). PRP studies have shown PRP to be so effective in the treatment of lateral epicondylitis that is now the standard of care (14). It enhances the healing of torn tendons, improves function, and reduces pain within the joint.
At the Centeno-Schultz Clinic (CSC), we are experts in the treatment of tennis elbow and golfer’s elbow. Under ultrasound guidance, super-concentrated PRP is injected into the areas of injury and tears to reduce swelling, promote healing and speed up recovery.
Board-certified, fellowship-trained physicians are available to evaluate your elbow pain besides assessing your shoulder and neck, as both may contribute to your elbow pain. Using the SANS approach, which evaluates the stability, symmetry, neurologic function, and articulation can optimize treatment recommendations and your clinical outcome.
Get The Right Treatment For Your Elbow Pain
Elbow pain can be debilitating. However, it is important to find out what is causing your elbow pain. The difference between a tennis elbow vs golfer’s elbow is one of location. Tennis elbow involves the lateral or outside of the elbow, whereas golfer’s elbow involves the inside of the elbow. Keep in mind they can occur simultaneously and to varying degrees of severity.
There are many treatment options including conservative care, and medications, including steroids and surgery. At CSC, our doctors are at the forefront of medicine, using regenerative therapy like PRP and bone marrow concentrate for elbow-related injuries.
Both can be effective, nonsurgical options that are the standard of care for lateral epicondylitis. It helps avoid the risks of surgery and extensive rehabilitation.
Don’t let elbow pain keep you on the sidelines. Let your own cells heal your ongoing elbow pain.
Are you a Candidate?
References:
- Taylor SA, Hannafin JA. Evaluation and management of elbow tendinopathy. Sports Health. 2012;4(5):384-93.
- Garg R, Adamson GJ, Dawson PA, Shankwiler JA, Pink MM. A prospective randomized study comparing a forearm strap brace versus a wrist splint for the treatment of lateral epicondylitis. J Shoulder Elbow Surg. 2010;19(4):508–512.
- Lai WC, Erickson BJ, Mlynarek RA, Wang D. Chronic lateral epicondylitis: challenges and solutions. Open Access J Sports Med. 2018;9:243-51.
- Prevalence and determinants of lateral and medial epicondylitis: a population study. Shiri R, Viikari-Juntura E, Varonen H, Heliövaara M Am J Epidemiol. 2006 Dec 1; 164(11):1065-74.
- David TS. Medial elbow pain in the throwing athlete. Orthopedics 2003;26:94-105.
- Barco R, Antuña SA. Medial elbow pain. EFORT Open Rev. 2017;2(8):362-71.
- George CE Sticking to the facts: A systematic review of the effects of therapeutic tape in lateral epicondylalgia. Phys Ther Sport. 2019 Aug 27;40:117-127. doi: 10.1016/j.ptsp.2019.08.011. PMID:31518778 https://www.ncbi.nlm.nih.gov/pubmed/31518778
- Russell B, Moss C, Rigg A, Van Hemelrijck M. COVID-19 and treatment with NSAIDs and corticosteroids: should we be limiting their use in the clinical setting. Ecancermedicalscience. 2020;14:1023.
- Pace CS Soft Tissue Atrophy Related to Corticosteroid Injection: Review of the Literature and Implications for Hand Surgeons. J Hand Surg Am. 2018 Jun;43(6):558-563. doi: 10.1016/j.jhsa.2018.03.004. Epub 2018 Apr 3. PMID: 29622410 https://www.ncbi.nlm.nih.gov/pubmed/29622410
- Reconstruction of the ulnar collateral ligament in athletes. Jobe FW, Stark H, Lombardo SJJ Bone Joint Surg Am. 1986 Oct; 68(8):1158-63.
- Donaldson CT Lateral Epicondylitis Debridement and Repair Using Knotless Suture Anchor. Arthrosc Tech. 2019 Jul 17;8(7):e775-e779. doi: 10.1016/j.eats.2019.03.016. eCollection 2019 Jul. PMID: 31485406 https://www.ncbi.nlm.nih.gov/pubmed/31485406
- Amroodi MN, Mahmuudi A, Salariyeh M, Amiri A. Surgical Treatment of Tennis Elbow; Minimal Incision Technique. Arch Bone Jt Surg. 2016;4(4):366–370. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5100454/
- Barnett J, Bernacki MN, Kainer JL, Smith HN, Zaharoff AM, Subramanian SK. The effects of regenerative injection therapy compared to corticosteroids for the treatment of lateral Epicondylitis: a systematic review and meta-analysis. Arch Physiother. 2019;9:12. Published 2019 Nov 13. doi:10.1186/s40945-019-0063-6