Have you had a neck injury or whiplash trauma? Do you have neck pain, especially when looking up, and you don’t know the cause? Then you may want to learn about the cervical anterior longitudinal ligament (ALL).
Anatomy of the Anterior Longitudinal Ligament
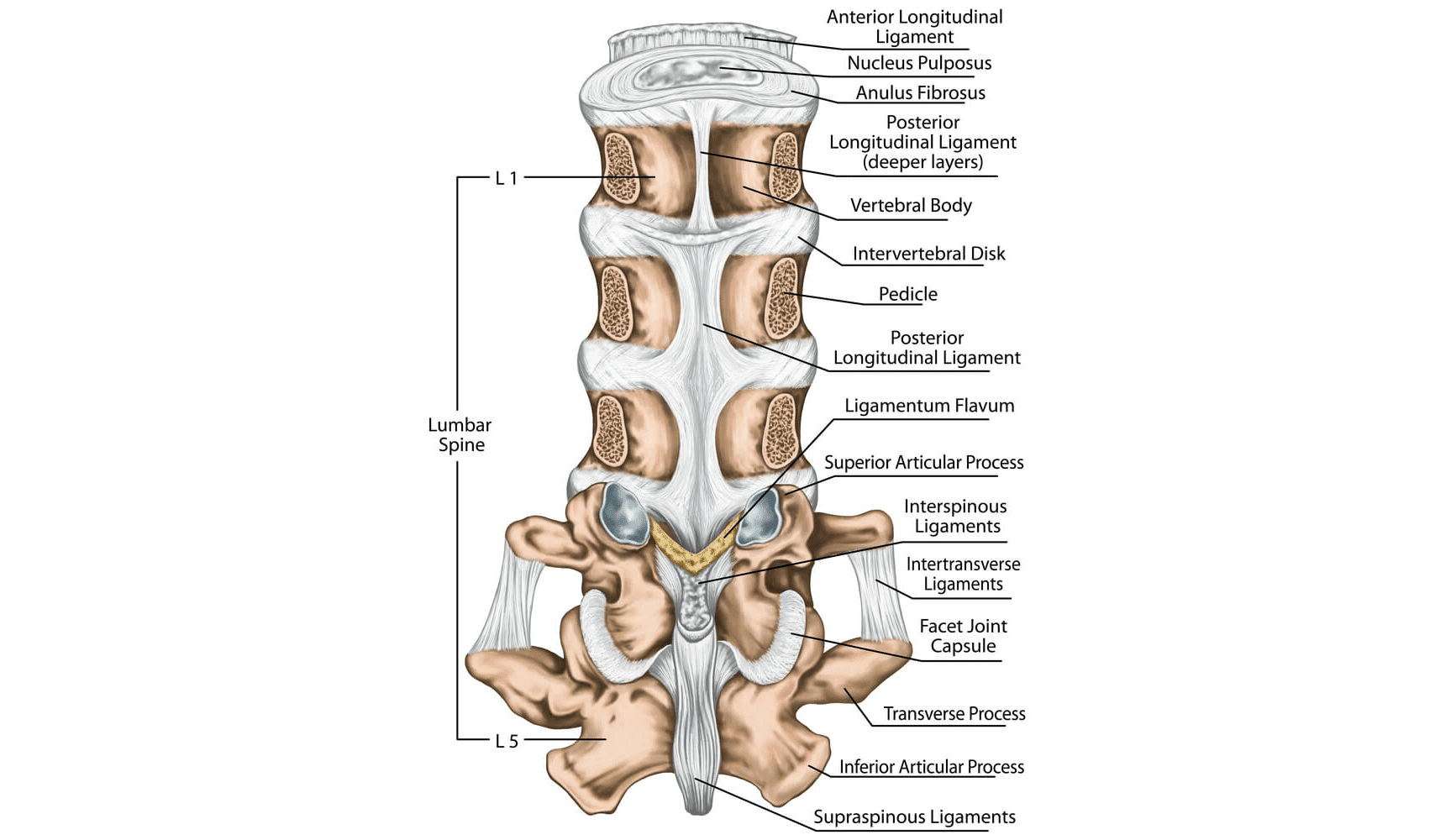
The ALL is a strong, wide ligament that runs along the front (anterior) of your spine. Ligaments are connective tissue that attach bone to bone to hold things in place.
Function of the Anterior Longitudinal Ligament
The function of the ALL is to resist excess spinal hyperextension. It helps to stabilize the front of the spine and confines and supports the intervertebral discs. Preventing hyperextension prevents excess stress on the posterior aspect of the disc and facet joints in the neck.
The ALL works in conjunction with a group of muscles called the longus colli in the front of the neck to maintain posture and prevent excess hyperextension.
Stabilizes the Front of the Spine
The ALL keeps the cervical vertebrae in proper alignment from the front. The ALL prevents the backward movement of the cervical vertebrae on the one below (retrolisthesis) in neck extension.
Limits Excess Neck Extension Motion
The ALL keeps pressure off the back neck structures such as the back (posterior discs) and facet joints.
Supports and Reinforces the Anterior Wall of the Disc
The ALL holds the disc in place from the front so it doesn’t bulge out toward the throat.
Why It’s Important to Keep This Ligament Healthy
It is important to keep this ligament healthy as it supports proper neck posture and alignment. Damage to this ligament can cause stress on the neck facet joints, posterior discs, and possibly spinal nerves.
Common Injuries Involving the Anterior Longitudinal Ligament
The most common cause of ALL ligament injuries is hyperextension or whiplash injuries.
Whiplash is a neck injury due to forceful, rapid back-and-forth whipping motion of the head and neck. The back motion typically injures the ALL, while the front motion can injure any of the many posterior (back) neck ligaments (1). The C5-6 ALL band is the most susceptible to injury (2).
ALL injuries usually occur along with other cervical injuries or chronic damage and can lead to other injuries such as facet joints, discs, muscles, tendons, and nerves, which can all be injured during whiplash. Commonly, the longus colli muscles, directly adjacent to the ALL, are damaged and inactive in whiplash injury as well (3).
- Spinal instability: A spine that moves too much will lead to wear and tear on its structures at a much quicker rate. When the vertebral bones are unstable due to ALL injury this causes spondylolisthesis or slippage of the bone on one another. This can cause less space around the spinal cord and cervical nerves.
- Spinal stenosis: Spinal stenosis is less space around the cervical spinal cord and nerves. This can be caused by ALL injuries, leading to instability. Spondylolisthesis, disc bulges, protrusions, facet joint arthritis that leads to hypertrophy (joint enlargement) and ligamentum flavum bulging can all lead to stenosis.
Stenosis can cause pain, numbness, tingling, and/or weakness in the neck and down the arms. In the most severe cases, it can cause spinal cord damage, which can affect breathing, the lower extremities, bladder function, and bowel function. - Disc injury: Cervical intervertebral discs can tear the outer fibers leading to disc bulges, protrusions, herniation, or extrusions. These can lead to spinal cord and cervical nerve irritation, which causes pain, numbness, tingling, and/or weakness in the neck and down the arms.
- Nerve injury: Spondylolisthesis, spinal stenosis, disc bulging, protrusion, herniations, and extrusions all can lead to nerve injury.
- Facet arthritis: The joints in the back of the neck can get stress from ALL ligament injuries. This stress leads to wear and tear on the joints and inflammation (arthritis) and leads to joint enlargement, called hypertrophy. Joint injuries can make the neck stiff and achy and contribute to spinal stenosis.
How to Diagnose ALL Injuries
The first step to diagnosing ALL ligament injury is seeing a board-certified musculoskeletal specialist who is familiar with this injury. The doctor should take a history and perform a physical examination. Common findings are pain in the neck with extension to other areas.
Imaging can provide more objective evidence of an ALL injury, but your doctor has to actively look for it as it is not something commonly discussed in an imaging report. Ligaments prevent excess motion, thus, to assess for instability or damage to a ligament you need movement-based imaging.
The best way to diagnose ALL injuries is with a digital motion X-ray (videofluoroscopy). A digital motion X-ray machine (DMX) takes X-ray pictures of a patient moving in different planes and takes measurements of how the bones move in relation to each other. If that movement is excessive, they suggest ligament injury.
The next best test would be flexion-extension X-rays or a flexion-extension MRI. On an X-ray, the physician can see a widening of the spaces in the front between the neck bones with the patient in neck extension compared to neutral, which suggests ALL injury.
Also, if a bone is sliding backward on the bone below it with extension, this is called retrolisthesis and suggests ALL injury. On an MRI, sometimes it is difficult to visualize the ALL directly, but sometimes you can see swelling in or around the ligament, suggestive of injury. Also, anterior disc bulging seen on MRI suggests ALL injury.
Conventional Treatment Approaches for ALL Injuries
When it comes to treating ALL injuries, several conventional approaches are commonly used. These approaches aim to promote healing and help individuals recover from their injuries. Here are some key points to consider:
- Physical therapy: Physical therapy plays a crucial role in rehabilitating ALL injuries. Therapists can design an exercise program to improve strength, flexibility, and posture, enhancing spinal muscular stability and function.
- Pain injections: Pain physicians can inject medications into areas that are painful secondary to the ALL injury. For instance, they can inject steroids around irritated nerves or inside irritated facet joints to temporarily reduce inflammation and decrease pain. These injections can help relieve pain so that you can participate in physical therapy. However, these injections do not help the underlying ALL injury. Also, repeated steroid injections have many risks and can actually inhibit the healing of tissues.
- Surgery: Surgery may be needed for the most severe ALL injuries that lead to spinal cord or nerve injury. Otherwise, surgery should be the last resort if all other conservative measures have failed.
- Non-invasive regenerative treatments: More recently there are newer regenerative treatments that can help ALL and associated injuries heal without drugs or surgery. These treatments involve precise injections of orthobiologics under ultrasound and/or X-ray guidance into damaged tissues to help them heal.
Orthobiologics are substances that help injured musculoskeletal tissues heal. The two most common examples are platelet-rich plasma (PRP) and bone marrow concentrate (BMAC), which contain stem cells.
At the Centeno-Schultz Clinic, we are experts in the diagnosis and treatment of orthopedic musculoskeletal problems, including neck pain and ALL injuries. We have 15 years of experience treating various neck problems such as the disc, facets, ligaments spinal nerves, tendons, etc., commonly with patients’ own PRP or stem cells.
In 2005, we were the first clinic in the world to inject stem cells into discs and we have been extensively using regenerative methods such as PRP and BMAC containing stem cells that contain growth factors that can improve the blood flow, reduce inflammation, accelerate healing and repair musculoskeletal tissues, thus resulting in less pain and improved function without the risk of steroid injections or major surgeries.
We use a functional spine unit approach instead of a pain generator approach. This means we look at the neck as a whole, treating all structures that are injured including the ALL when appropriate. In fact, we pioneered an approach to safely and accurately inject the cervical ALL under ultrasound and X-ray guidance.
A Vital Partner in Your Spine’s Health
The ALL plays a vital role in maintaining spine health and overall well-being. Its function of stabilizing the front of the spine and supporting the intervertebral discs is crucial for proper alignment and posture. Ignoring symptoms that could be attributed to injuries of the ALL can lead to various complications such as spinal instability, spinal stenosis, disc injuries, nerve damage, and facet arthritis.
It is essential to prioritize the health of this ligament and seek appropriate medical attention if any related symptoms arise. By understanding the significance of the ALL and taking necessary precautions, we can ensure a healthier and pain-free spine.
Learn about the common injuries involving the anterior longitudinal ligament and how to get the best treatment to address your condition.
References:
- Pastakia K, Kumar S. Acute whiplash associated disorders (WAD). Open Access Emerg Med. 2011;3:29-32. Published 2011 Apr 27. doi:10.2147/OAEM.S17853.
- Stemper BD, Yoganandan N, Pintar FA, Rao RD. Anterior longitudinal ligament injuries in whiplash may lead to cervical instability. Med Eng Phys. 2006;28(6):515–524. doi:10.1016/j.medengphy.2005.09.011
- Jull, GA. Deep Cervical Flexor Muscle Dysfunction in Whiplash. 2000, Vol. 8, No. 1-2 , Pages 143-154