Could Craniocervical Instability Be the Cause of Your Symptoms?
Imaging-Get movement based imaging (DMX or Upright MRI with flexion and extension).

Get Typed via a Telemed Appointment-There are 8 different types of CCI based on which ligaments are Injured.

Exam-If you’re a candidate for precise orthobiologic injections, you fly in for an exam and treatment. A hands-on exam refines what we need to treat.
Treatment-Get treated with a CCI focused, orthobiologic treatment plan tailored to you. That includes PICL or whichever image guided, precise injections are the most likely to help you.
Tackles were part of every weekend’s football and rugby game. Early on the aches and pain were minor and always resolved. Unfortunately, over time the neck pain, headaches, and dizziness did not improve. They actually got worse. Rest and physical therapy did not help. Your doctor is considering a referral to a surgeon. What is Craniocervical Instability? What is the Alar ligament? What are the symptoms of Craniocervical Instability? What are Craniocervical Instability treatment options? What is Craniocervical Instability surgery? What regenerative treatment options exist? Meet BR who avoided Craniocervical Instability surgery. Let’s dig in.
What Is Craniocervical Instability?
Neck ligament laxity, also known as Cranial Cervical Instability (CCI) is a medical condition where the strong ligaments that hold your head to your upper neck are loose or lax (1). The major ligaments involved are the Alar, Transverse and Accessory ligaments. To learn more about CCI please click on the video below.
What Is the Alar Ligament? (Ligament that Holds Your Head onto Your Neck)
Ligaments are thick bands of connective tissue that connect one bone to another. The Alar ligament is in the upper portion of the cervical spine and connects the upper neck to your head. There is a right and a left Alar ligament which is illustrated to the right. The Alar ligament provides critical stability for your head and neck. It holds your head onto your neck.
What Are the Symptoms of Craniocervical Instability? (8 Most Common)
Excessive movement between your head and neck can cause movement and damage of the upper cervical facet joints, discs, nerves, and blood vessels. Symptoms vary depending upon the amount of instability. Common Craniocervical Instability symptoms include:
1. Painful, Heavy Head
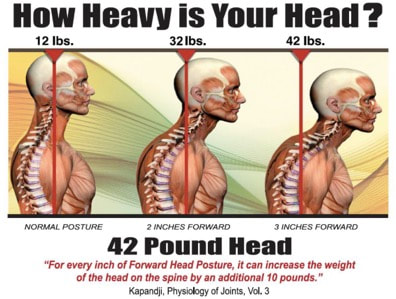
A constant to near-constant head pain can be described as feeling like the head is too heavy for the neck to support. Many describe feeling like they have a “bobblehead”. Neck weakness along with ligament instability results in head forward posture in many patients. This has significant consequences as the weight of your head dramatically increases as it moves forward from neutral alignment. This is illustrated below. On the left, in neutral spinal alignment, your head weighs 12 lbs. With just 2 inches forward posture the weight of the head increases to 32lbs. Add another 1 inch forward and the weight increases to 42lbs. This is an enormous amount of weight that can not be sustained or supported. Pain, limitation, and compromised posture ensures and curve of the thoracic spine starts (kyphosis)
2. Headache
This is not your normal headache caused by your in-laws or excessive consumption of alcohol. This is a debilitating headache that is constant in duration and miserable. Headache is often caused by the upper neck joints, muscles, and tendons getting injured due to ongoing instability.
3. Rapid Heart Rate
Elevated heart rate may occur as the vagus nerve gets irritated by the extra motion in the upper neck. Another cause of elevated heart rate is Postural Orthostatic Tachycardia Syndrome (POTS). POTS is a medical condition that causes malfunction of the autonomic nervous system. It is estimated to impact between 1,000,000 and 3,000,000 Americans. The autonomic nervous system controls involuntary body functions such as heart rate and blood pressure. Malfunction of the autonomic nervous system causes a number of symptoms which include rapid heart rate.
4. Brain Fog
Patients with CCI can struggle with memory, concentration, and ability to complete tasks. Every day can feel like your brain is stuffed full of cotton.
5. Neck Pain
Pain is typically localized at the base of the skull and aggravated with flexion and rotation. The pain can shoot up into the base of the skull, top of the head, frontal area or behind the eyes.
6. Visual Problems
Visual disturbances can vary from mild to severe involving a number of symptoms. Visual disturbances can happen because the upper neck supplies information to the brain to guide eye position and vice versa (2).
7. Dizziness
Balance problems can be a significant issue (3). Dizziness or imbalance is a feature related to the fact that the upper neck is a major contributor to balance (4). The upper neck provides position sense that has to be coordinated with balance information from the eyes and inner ear.

8. Chronic Fatigue
Excessive movement between the head and neck can cause irritation and dysfunction of the nervous system. The autonomic nervous system is the most affected. A common symptom of autonomic dysfunction is chronic fatigue.
What Causes of Craniocervical Instability? (Trauma and Hypermobility)
Trauma
Whether it is one major event or a series of repetitive traumas over time, trauma to the cervical spine can cause cervical instability. For example during a motor vehicle accident ligaments in the neck can be overextended, disrupted and injured leading to chronic cervical instability. Other examples include sports injuries or forceful chiropractic adjustments (5).
Inflammatory Conditions
Chronic inflammatory diseases can be debilitating. In such cases, a patient’s own immune system attacks itself resulting in inflammation, injury, and pain. Common examples include rheumatoid arthritis, scleroderma, and lupus. Patients with rheumatoid arthritis are at risk for Cranial Cervical Instability.
Congenital
Congenital disorders are also known as birth defects. There are many different types of birth defects which include cleft lip, cerebral palsy, and Down’s syndrome. Patients with Down’s syndrome are a risk for CCI (6).
Connective Tissue Disorders
There are a number of medical conditions where the ligaments are loose due to defects in the connective tissue. These patients have overly flexible joints that allow them to very, very flexible. Ehlers Danlos Syndrome is a classic example of such patients (7). There are thirteen different subtypes. Symptoms can vary depending upon the severity of the condition. Patients with EDS can easily bend their thumbs backward so that they can touch their forearms. EDS patients due to their loose ligaments are a risk for Cranial Cervical Instability.
Craniocervical Instability Treatment Options: Conservative Care, Injections and Surgery
Treatment of Ehlers-Danlos syndrome-related Craniocervical Instability is challenging. Not having an accurate diagnosis can make it even more challenging. A lack of diagnosis can send patients on a many-year journey looking for assistance. Some will be dismissed as their complaints are considered not valid or genuine whereas others will be labeled “hormonal”, anxious or psychiatric and referred elsewhere or medicated with anti-depressants, opioids, or anti-anxiety medications. There are three major types of CCI treatments: conservative care, injections and Craniocervical Instability Surgery. The specific type of treatment will depend upon the amount of instability and a patient’s clinical presentation.
Conservative Care
Patients with small amounts of instability can oftentimes be managed with conservative care. Treatment options include:
1. Upper cervical chiropractic care. Look for members of NUCCA (National Upper Cervical Chiropractic Association)
2. Physical Therapy
3. Bracing
4. Curve restoration. Look for chiropractors that specialize: Chiropractic BioPhysics or CBP is a protocol utilized by a select group of chiropractors who look to spinal rehabilitation and postural correction as a means to address pain, disease, and dysfunction.
Traditional Injections
Precise x-ray guided injections with PRP or bone marrow concentrate (BMC), containing stem cells, are the next treatment options for those patients who fail to receive any clinical benefit from conservative care. Examples include
C0/1 and C1/2 facet injections.
A facet is a paired joint on the backside of the spine that provides support and limits rotation of the spine. It can also be irritated or injured causing significant neck and head pain (7). Few clinics perform this injection due to the skill required.
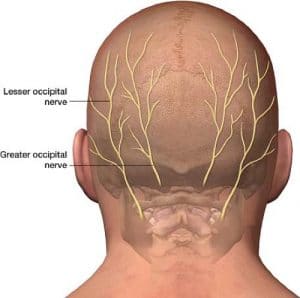
Occipitals Nerve block.
The occipital nerves arise from the upper cervical spine and travel up into the back of the head. There is one nerve on each side of the head. When irritated, injured, or compressed they can cause significant pain in the back and top of the head (8).
Superficial cervical plexus injection
Ligament injections to stabilize injured or lax ligaments.
Ligaments are thick pieces of connective tissue that connect bone to bone. Loose or damaged ligaments can cause significant instability, pain, and dysfunction.
Surgery
See below
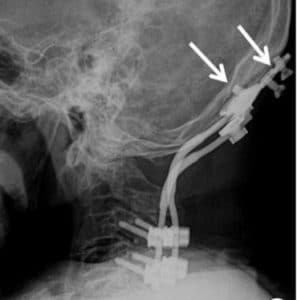
What is Craniocervical Instability Surgery?
Craniocervical Instability Surgery always involves a fusion. Fusion is a surgical procedure where one or more of the bones in the spine are joined together by screws, bolts, and rods. The hardware provides mechanical stability. In most cases of Craniocervical Instability, the upper portion of the neck (C1 and C2 vertebral bodies) is fused to the skull. The skull is also called the occiput. The surgery can also be called an occipitocervical fusion. This is major surgery and rehabilitation. The procedure depending on the complexity typically ranges from 130-320 minutes (9).
The upper cervical spine is a very complex area rich in nerves, arteries, veins, ligaments, tendons, and muscles. The risks associated with upper neck fusion are significant and include (9):
Screw failure: The screw that is inserted into the occiput or C1 or C2 can fracture, bend or break. In most cases surgical revision is necessary.
Screw loosening: The implanted screw can back out of the bone over time compromising the stability of the upper neck.
Infection: The infection can be localized to the skin or may penetrate deeper into the muscles or bone. Antibiotics are oftentimes required for skin infections. Bone infections require additional surgery.
Vertebral artery injury: The vertebral artery provides critical blood flow to the spinal cord and brain. The artery can be compressed, irritated, or injured during the surgery.
Spinal Cord Injury: The spinal cord runs from the base of the head to the lower back and contains critical nerve tissue that controls the central nervous system.
Cervical Facet Injury: The screw can be advanced into the facet joint thereby injuring the joint cartilage leading to arthritis, pain, and restriction in range of motion.
Upper Neck Muscle Weakness: The muscles can be injured during the surgical fusion.
Dural Leak: The dura is a thin layer of connective tissue that covers the brain and spinal cord. It can be injured during the surgery resulting in leakage of spinal fluid (10).
Hematoma: A collection of blood that can compress or injure nerves, arteries, and veins
Persistent upper cervical instability requiring additional surgery .(11)
Limited Neck Range of Motion: Fusion of the skull base to the upper neck can severely restrict the range of motion in the upper neck.
Adjacent Segment Disease ( ASD): Fusion of the spine significantly alters the biomechanics of the spine. The fused segment is no longer able to absorb the forces of daily living. As such these forces are then transferred above and below the fusion. This additional force can overload the discs, facet joints, muscle, and ligaments above and below the fusion which start to break down. To learn more about adjacent segment disease please click on the video below.
Regenerative Treatment Options
In 2015 a nonsurgical treatment option for Cranial Cervical Instability was developed at the Centeno-Schultz Clinic. It involves the injection of a patient’s own bone marrow concentrate into the damaged alar and transverse ligaments. The procedure is called Percutaneous Implantation of Cervical Ligaments (PICL) It is a very demanding procedure and is only performed at the Centeno-Schultz Clinic in Broomfield Colorado. To learn more about this groundbreaking procedure please click on the video below.
Meet BR
BR is a 19y/o accounting student from the United Kingdom with documented Craniocervical Instability after multiple athletic and ruby related injuries, He had ongoing neck pain that was constant in duration, 4 out of 10 in severity localized in the upper cervical area with debilitating headaches behind his eyes, forehead, and top of the head. He also had lower neck pain radiating into the shoulder and both hands with intermittent numbness and tingling. Neurologic symptoms that accompanied his neck pain included brain fog, dizziness, difficulty with word selection, blurred vision, anxiety, and elevated heart rate. BR had undergone extensive treatment without clinical benefit. Treatments included rest, ice, heat, physical therapy, supplements, and NUCCA chiropractic care. He had exhausted all conservative treatment options available in the UK. He was evaluated by surgeons and was identified as a candidate for cervical fusion. BR declined surgery and opted to use his own BMC at the Centeno-Schultz Clinic. In December 2020, BR underwent the PICL procedure with precise injection of his BMC into the alar and transverse ligaments. At 4 months post-procedure, he has noted a profound reduction in both his neck pain and neurologic symptoms.
In Conclusion
- Craniocervical Instability is a medical condition characterized by injury and instability of the ligaments that hold your head onto the neck.
- Common symptoms of Cranial Cervical Instability include a painful, heavy head, headache, rapid heart rate, brain fog, neck pain, visual problems, dizziness, and chronic fatigue.
- Trauma is the most common cause of CCI however patients with hypermobility are at risk.
- CCI or neck ligament laxity treatment options depend upon the severity of the instability and clinical symptoms. When appropriate, conservative care should always be the first-line treatment.
- Cranicervical Instability Surgery is often recommended when conservative care fails. This involves a fusion of the head to the neck which is a major surgery that is associated with significant risks and complications.
- The PICL procedure is a revolutionary non-surgical craniocervical instability treatment option where a patient’s own bone marrow concentrate, containing stem cells, is injected into the damaged upper cervical ligaments.
- BR successfully avoided Craniocervical Instability surgery by having his BMC injected into his damaged alar and transverse ligaments at the Centeno-Schultz Clinic.
If you or a loved one has sustained an injury with ongoing headaches, neck pain, and brain fog please schedule a telephone candidacy discussion with a board-certified, fellowship-trained physician. From the comfort of your home or office learn what treatment options are available for you. Call today and stop the pain, misery, and suffering.
1.Offiah CE, Day E. The craniocervical junction: embryology, anatomy, biomechanics and imaging in blunt trauma. Insights Imaging. 2017;8(1):29–47. doi:10.1007/s13244-016-0530-5
2.Sobey G. Ehlers-Danlos syndrome – a commonly misunderstood group of conditions. Clin Med (Lond). 2014;14(4):432-436. doi:10.7861/clinmedicine.14-4-432
3.Biesinger E. and Vertigo caused by disorders of the cervical vertebral column. Diagnosis and treatment. Adv Otorhinolaryngol. 1988; 39: 44– 51.
4.Thompson-Harvey A, Hain TC. Symptoms in cervical vertigo. Laryngoscope Investig Otolaryngol. 2018;4(1):109–115. Published 2018 Nov 28. doi:10.1002/lio2.227
5.Henderson FC Sr, Francomano CA, Koby M, Tuchman K, Adcock J, Patel S. Cervical medullary syndrome secondary to craniocervical instability and ventral brainstem compression in hereditary hypermobility connective tissue disorders: 5-year follow-up after craniocervical reduction, fusion, and stabilization. Neurosurg Rev. 2019;42(4):915-936. doi:10.1007/s10143-018-01070-4
6.Ashafai, Nabeel S.; Visocchi, Massimiliano; Wąsik, Norbert (2019). “Occipitocervical Fusion: An Updated Review“. Acta Neurochirurgica. Supplement. 125: 247–252. doi:10.1007/978-3-319-62515-7_35. ISSN 0065-1419. PMID 30610329.
7.Manchikanti L, Boswell MV, Singh V, Pampati V, Damron KS, Beyer CD. Prevalence of facet joint pain in chronic spinal pain of cervical, thoracic, and lumbar regions. BMC Musculoskelet Disord. 2004;5:15. Published 2004 May 28. doi:10.1186/1471-2474-5-15
8. Juškys R, Šustickas G. Effectiveness of treatment of occipital neuralgia using the nerve block technique: a prospective analysis of 44 patients. Acta Med Litu. 2018;25(2):53-60. doi:10.6001/actamedica.v25i2.3757
9. Mazur MD, Ravindra VM, Brockmeyer DL. Unilateral fixation for treatment of occipitocervical instability in children with congenital vertebral anomalies of the craniocervical junction. Neurosurg Focus. 2015 Apr;38(4):E9. doi: 10.3171/2015.1.FOCUS14787. PMID: 25828503.
10.Upadhyaya M, Jain S, Kire N, Merchant Z, Kundnani V, Patel A. Surgical, clinical, and radiological outcomes of occipitocervical fusion using the plate-screw-rod system with allograft in craniocervical instability. J Craniovertebr Junction Spine. 2019;10(4):216-223. doi:10.4103/jcvjs.JCVJS_87_19
11.Wenning, K.E., Hoffmann, M.F. Does isolated atlantoaxial fusion result in better clinical outcome compared to occipitocervical fusion?. J Orthop Surg Res 15, 8 (2020). https://doi.org/10.1186/s13018-019-1525-y
Am I a Candidate?
To answer this question, fill out the candidate form below to request a new patient evaluation, and a patient advocate will reach out to you to determine your next steps. Your one-hour, in-office or telemedicine evaluation will be with one of the world’s experts in the field of Interventional Orthopedics.