Hip pain can be debilitating eroding one’s function and quality of life. What is the hip labrum? What is hip labrum surgery? What is hip labrum surgery recovery? Let’s dig in.
What is Hip Labrum?
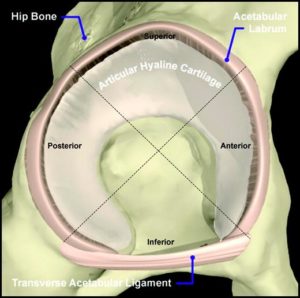
The hip joint is a ball-socket joint with the acetabulum being the shallow socket. The labrum is a ring of fibrocartilage and connective tissue attached to the acetabulum. The labrum provides support to the hip, deepens the shallow joint and increases the surface area of the acetabulum by 28% (1). Tears in the hip labrum can occur as a result of direct trauma and activities that require external rotation such as soccer, hockey, and golf. Unfortunately, up to 74% of all hip labrum tears are not associated with any known specific cause or event (2). Labral tears are reported more in females than males (3).
Pain can be a common complaint typically localized in the anterior hip or groin. Other mechanical symptoms may be present which include clicking, locking or giving away.
What is Hip Labrum Surgery?
Hip labrum surgery involves the insertion of a narrow-gauge camera and operating instruments into the hip joint. This is called arthroscopy and allows the surgeon to visualize structures inside of the hip joint including the labrum. Small labral tears are some times “repaired” with stitches. More commonly there is debridement which involves removing a portion of the labrum. There has been a rapid increase in the number of hip arthroscopies in the United States over the last 20 years. From 2007 to 2014 the number increased by 117% (4). The insertion of the surgical camera and instruments into the small, tight hip joint requires partial dislocation of the joint by means of a traction table. The most common complication of hip labrum surgery is nerve damage with an incidence of 16.5% (5). Nerve damage is more common in women than men and increases with longer traction times.
Post Surgery Guidelines
Hip labrum surgery recovery involves rehabilitation which is divided into four phases.
Phase 1: weeks 1-4: 50% partial weight-bearing for 10 days or more and light strengthening. The goal is to minimize inflammation, protect the surgically repaired tissue and control pain. Narcotics are frequently needed.
Phase 2: weeks 5-7: Focus is to improve range of motion and flexibility through extensive physical therapy.
Phase 3: weeks 8-12: Focus is on symmetrical range of motion and integrated functional strengthening. Multi-planar movements and strengthening with multiple muscle groups are important.
Phase 4: weeks 12 and beyond: Focus is on safe return to competition or previous activity level utilizing manual therapy, flexibility, and range of motion exercises.
Little evidence exists in the current literature to support rehabilitation procedures after hip labrum surgery (6). Twelve weeks of extensive physical therapy and strengthening is a significant investment in time and money. This is in addition the downtime due to pain and immobility that patients experience.
Is Hip Labrum Surgery Successful?
A recent study at Mayo Clinic followed 57 patients who underwent surgery for labral tears. An alarming 45% of patients had poor clinical results at an average of 5 years after the surgery (7). 20% of patients required additional surgery. In a different study, 80 patients with documented labral tears were randomized to undergo surgical repair or physical therapy. At 2 years there was no difference in outcomes between the two groups. Hip labral surgery was no better physical therapy (8). In a review of multiple research studies examining pain and hip function after hip surgery for patients with FAI, authors demonstrated more pain and less function in the surgical group as compared to nonsurgical counterparts (9).
Another important concern is whether or not labral tears cause pain. A 2013 study looked at the MRIs of 85 patients with hip pain and found no association between pain and labral tears (10). A different study followed professional Danish ballet dancers. It demonstrated that those with pain while dancing had no more evidence of labral tears on MRI than those dancers without hip pain (11). Is it possible to have a labral tear and no pain? Yes! Another study looked at 45 patients, with an average age of 38 years with no hip pain and found that 69% had labral tears (12).
Platelet-rich plasma (PRP) injections have been effective in the treatment of labral tears with a reduction of pain and improved function at 8 weeks (13). Bone marrow-derived stem cells injected into labral tears have also resulted in a reduction in pain (14). At the Centeno-Schultz Clinic, we pioneered orthopedic stem cell injections and have extensive experience in the treatment of hip labral tears. The injection of a labral tear is not a procedure that your family physician, or surgeon, can perform.. The labrum is a small structure and demands significant skill and training to inject. All injections are performed under x-ray or ultrasound guidance or both. To better understand the complexity of stem cell injections in the labral please click on the video below.
https://www.youtube.com/watch?v=Gdrwf2-Tw8I
To Conclude…
The hip labrum is a ring of fibrocartilage that provides support and reduces stress within the hip joint. It is susceptible to injury and often with no specific event or trauma. The presence of a labral tear on MRI is not correlated with pain. Surgery involves repair or excision of the damaged tissue and has become increasingly popular. Traction is required and is associated with nerve injuries. Studies have demonstrated labral surgery to be no better than PT and reduced function. Platelet-rich plasma and stem cells are effective treatment options without the associated risks, extensive rehabilitation and complications associated with surgery.
Tan V, Seldes RM, Katz MA, Freedhand AM, Klimkiewicz JJ, Fitzgerald RH. Contribution of acetabular labrum to articulating surface area and femoral head coverage in adult hip joints: an anatomic study in cadavera. Am J Orthop. 2001;30(11):809-12.
Santori N, Villar RN. Acetabular labral tears: result of arthroscopic partial limbectomy. Arthroscopy. 2000;16(1):11-5.DOI: 10.1016/s0749-8063(00)90121-x
Dorrell JH, Catterall A. The torn acetabular labrum. J Bone Joint Surg Br. 1986;68(3):400-3.
Truntzer JN, Shapiro LM, Hoppe DJ, Abrams GD, Safran MR. Hip arthroscopy in the United States: an update following coding changes in 2011. J Hip Preserv Surg. 2017;4(3):250-7.doi: 10.1093/jhps/hnx004
Larson CM, Clohisy JC, Beaulé PE, et al. Intraoperative and Early Postoperative Complications After Hip Arthroscopic Surgery: A Prospective Multicenter Trial Utilizing a Validated Grading Scheme. Am J Sports Med. 2016;44(9):2292-8.DOI: 10.1177/0363546516650885
Garrison JC, Osler MT, Singleton SB. Rehabilitation after arthroscopy of an acetabular labral tear. N Am J Sports Phys Ther. 2007;2(4):241-50.
Krych AJ, Kuzma SA, Kovachevich R, Hudgens JL, Stuart MJ, Levy BA. Modest mid-term outcomes after isolated arthroscopic debridement of acetabular labral tears. Knee Surg Sports Traumatol Arthrosc. 2014;22(4):763-7.DOI: 10.1007/s00167-014-2872-1
Mansell NS, Rhon DI, Marchant BG, Slevin JM, Meyer JL. Two-year outcomes after arthroscopic surgery compared to physical therapy for femoracetabular impingement: A protocol for a randomized clinical trial. BMC Musculoskelet Disord. 2016;17:60.doi: 10.1186/s12891-016-0914-1
Kierkegaard S, Langeskov-Christensen M, Lund B, et al. Pain, activities of daily living and sport function at different time points after hip arthroscopy in patients with femoroacetabular impingement: a systematic review with meta-analysis. Br J Sports Med. 2017;51(7):572-9.DOI: 10.1136/bjsports-2016-096618
Krych AJ, Kuzma SA, Kovachevich R, Hudgens JL, Stuart MJ, Levy BA. Modest mid-term outcomes after isolated arthroscopic debridement of acetabular labral tears. Knee Surg Sports Traumatol Arthrosc. 2014;22(4):763-7.DOI: 10.1007/s00167-014-2872-1
Duthon VB, Charbonnier C, Kolo FC, et al. Correlation of clinical and magnetic resonance imaging findings in hips of elite female ballet dancers. Arthroscopy. 2013;29(3):411-9.DOI: 10.1016/j.arthro.2012.10.012
Register B, Pennock AT, Ho CP, Strickland CD, Lawand A, Philippon MJ. Prevalence of abnormal hip findings in asymptomatic participants: a prospective, blinded study. Am J Sports Med. 2012;40(12):2720-4.DOI: 10.1177/0363546512462124
De Luigi AJ, Blatz D, Karam C, Gustin Z, Gordon A. Use of Platelet Rich Plasma for the Treatment of Acetabular Labral Tear of the Hip: A Pilot Study. Am J Phys Med Rehabil. [published online: May 30, 2019]. 10.1097/PHM.0000000000001237
Garwood ER, Burke CJ, Jazrawi LM, Adler RS. Percutaneous Ultrasound-Guided Musculoskeletal Applications of Autologous Bone Marrow Aspirate Concentrate: Preliminary Experience From a Single Institution. Ultrasound Q. 2018;34(4):278-84.DOI:10.1097/RUQ.0000000000000339