With spring giving way to summer next week and Wimbledon just around the corner, we are in the midst of tennis season, when tennis courts everywhere stay busy with athletes in training and weekend warriors alike. While the term “tennis elbow” may lead you to believe it is a risk of the game, the truth is you don’t have to be a tennis player to get tennis elbow. In fact, while we do sometimes find tennis elbow in those with occupations that require highly repetitive elbow motions (such as factory-line workers), we more commonly find it in middle-aged people who suddenly experience elbow pain. Why? We’ll answer this question in a moment, but let’s first define this condition.
Tennis Elbow and the Lateral Epicondyle
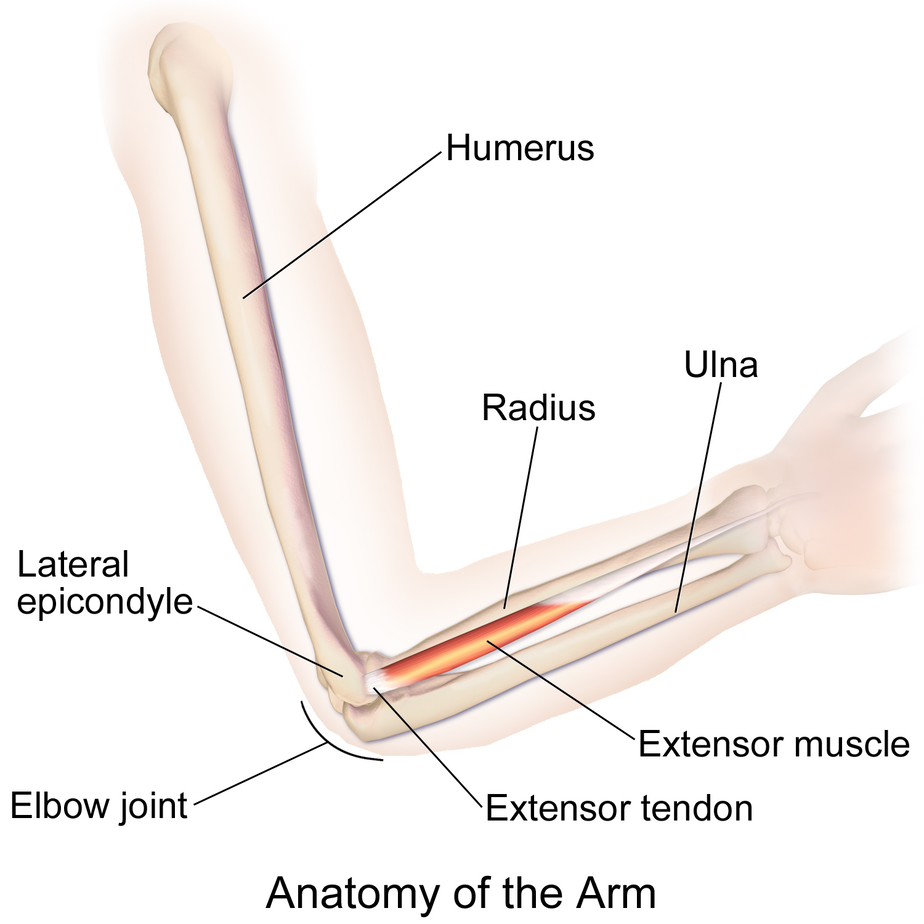
The lateral epicondyle is a structure located at the distal end (the elbow end) of the humerus (the upper-arm bone). Lift your arm out in front of you with your palms facing up. Bend your elbow about 90 degrees. The first structure you’ll likely notice when you touch your bent elbow is the olecranon, the large knob-like prominence located directly at the 90-degree angle. This is actually the elbow end of the ulna (the larger lower-arm bone). Slide your fingers toward the thumb side of your elbow, and you’ll feel another bony prominence. This is your lateral epicondyle.
Lateral epicondylitis is the medical terminology for the common phrase “tennis elbow.” The lateral epicondyle is the attachment point for tendons that extend the wrist and fingers, and when these tendons degenerate or tear, this is lateral epicondylitis. While the -itis suffix in epicondylitis actually means inflammation, we now know this type of tendinopathy isn’t about inflammation, as once thought, but about the degenerated or torn tendon.
What Causes Tennis Elbow?
To understand tennis elbow, you have to understand the interconnected body and how every specialized part works together to create one fully functioning body machine. On the surface, your neck may not seem like it would have anything to do with your elbow; however, the nerve system that supplies the upper extremity, from the shoulder all the way down to the tips of the fingers, branches off of the cervical spine in the neck, making the neck a critical part of the function of the elbow. So when the elbow is painful, it is imperative that an examination extend beyond the elbow and include the shoulder and neck complex as well.
We mentioned earlier that we more commonly see tennis elbow in middle-aged people who have experienced sudden elbow pain. What we most often discover is these patients have nerve irritation in the neck that is presenting as referred pain at the elbow branch of the nerve. When the nerve signals aren’t properly functioning along this branch, the forearm muscles can put too much force on the tendon attachments at the lateral epicondyle, hence, tennis elbow. Despite the irritated neck nerve, you may not feel any pain or discomfort in the neck; tennis elbow may be your early-warning signal. Addressing that early warning signal is key to preventing further problems later.
Treatment Options to Avoid for Tennis Elbow
One treatment option to avoid is tennis elbow surgery, which has been shown to be no better than a sham surgery. This surgery attempts to stimulate healing by placing small perforations in the tendon. Thankfully, since studies have found less-invasive options to be more effective, the number of tennis elbow surgeries have been dropping for many years, so hopefully at this point it’s not something your doctor is quickly recommending. And since, so often, tennis elbow is actually due to a nerve issue in the neck, elbow surgery would certainly be counterproductive.
Extracorporeal shock wave therapy also hasn’t fared well in some of the research literature on tennis elbow. This involves immersing the arm in a water tank and aiming sound waves at the injured area to create tissue disruption.
Treatment Options to Consider for Tennis Elbow
Platelet-rich plasma (PRP) injections have been shown via a large randomized controlled trail to be effective options for tennis elbow. Blood is taken from an arm vein, and then the patient’s platelets are concentrated and reinjected under precise image guidance into the painful tendon. If the tendon injury is more extreme (rare), an injection of bone marrow stem cells may also be an option. An interventional orthopedic physician will also examine the neck and shoulder, and if the tennis elbow is due to an irritated nerve, the source of this irritation (e.g., disc issues, spinal stenosis, etc.) can be treated with orthobiologics as well.
In our experience prolotherapy can also be effective. This involves injecting a solution that creates a brief inflammatory healing reaction. If the tennis elbow is truly sourced in the elbow itself and not due to something bigger, like an irritated neck nerve, physical therapy and time may be all that is needed to eliminate pain and restore elbow function.
Tennis elbow isn’t always a true elbow problem. If you have elbow pain, make sure your physician is also examining your neck and elbow to determine the true source of the problem. Surgery, steroids, and shock wave therapy should be avoided as there are other solutions, such as your own PRP, available that can address tennis elbow as well as irritated neck nerves if they are the source.
Learn more about your elbow condition and how Interventional Orthopedics can prevent the need for surgery by reading Orthopedics 2.0.