The Trusted Knee Replacement Alternative
Regenexx Treatment for Knee Osteoarthritis
What is the Percutaneous Knee Arthroplasty?
Knee pain keeping you down and out? It is incredibly common for physicians to recommend knee replacement surgery as a remedy for lasting, cumbersome, or debilitating knee pain as a treatment for knee osteoarthritis. Also called Total Knee Arthroplasty (or TKA), knee replacement surgery involves the surgeon amputating or cutting out the existing knee joint, reaming the bone, and inserting a prosthetic device in place of the natural joint (1). Alternatively, a doctor may opt to replace small parts of the joint, such as the medial, lateral, or anterior compartments, as opposed to a total knee replacement. It’s important to keep in mind if you have had knee replacement surgery recommended to you by your physician, that this surgery is not without its risks and side effects.
Patients with knee arthritis can also be treated with a newer procedure called Percutaneous Knee Arthroplasty, or Perc-Knee Arthroplasty or PKA for short. In this procedure, the physician injects the joints and lax ligaments, damaged meniscus tissue, and tendons with your own body’s stem cell-rich bone marrow concentrate or blood platelets (platelet-rich plasma or platelet lysate). And it is important to note that the PKA is a precise ultrasound and fluoroscopy-guided procedure, as opposed to a quick knee shot. It has been shown to be effective in randomized, controlled trials, and appears to work well whether or not the knee arthritis is severe (21). This procedure generally is effective for two to seven years at a time, at which point it often needs to be repeated. Of all knee replacement surgery alternatives, the PKA procedure seems to be a solid choice that helps more than hurts in the long run.

Participate in the Stem Cell Support Formula Study for Patients with Knee Osteoarthritis
The Centeno-Schultz Clinic and Regenexx are investigating whether our stem cell support supplement (Advanced Stem Cell Support Formula) provides improvement in joint health for those suffering with knee osteoarthritis.
Knee Replacement vs. The PKA
What are the risks involved in knee replacement?
Unfortunately, knee replacement surgery is no small task. This procedure is a large-scale, invasive surgery that comes with some pretty notable risks that you should understand before agreeing to it. These risks include:
- *A dramatically increased risk of heart attack or stroke immediately post-surgery (9, 10)
- *Metal ions could end up in your bloodstream (4-6)
- *You may end up having an allergic reaction to the metal in the prosthesis (7, 8)
*Infection after surgery is possible (22)
Make sure that you understand and are comfortable with the risks involved with knee replacement before choosing to undergo the procedure. It is advised to find a non-surgical knee treatment, and Regenexx’s non-surgical knee osteoarthritis treatment is one such procedure.
Even with knee replacement surgery, your knee pain may not go away
If you thought that the whole point of knee replacement surgery was to solve the problem of knee pain, you would be right. Which is why it should come as a surprise to patients when they find that a sizeable population of those who have undergone knee replacement surgery still have knee pain after the surgery is completed. In one recent study, nearly 40% of patients who had gone through the invasive surgery reported that they still had pain ranked between 3 and 5 on a 10-point scale, despite having their knee replaced (2). In yet another study, 44% of knee replacement surgery patients still had moderate pain three to four years post-surgery (3).
If you are under the impression that surgery will be a certain, complete resolution of your problems with knee pain, you may need to think again. Based on the research, you may find an alternative to be a better option.
In the video below, Dr. Chris Centeno goes over the results of a large randomized control trial for total knee replacement and his take on the results:
Post-surgery activity levels may not ever improve
You may have seen the commercials: People in the prime of their retirement years smiling, riding their bicycles, climbing mountains, jogging through their neighborhood, or doing something equally active after knee replacement, all thanks to their new knee. However, the reality based on published patient data tells an entirely different story.
One government-funded study found that there was no increase in activity for patients who had undergone knee replacement surgery (11), and another showed that if patients were not running regularly before knee replacement surgery, it was incredibly unlikely that they would run regularly after the procedure was done. Very few patients actually markedly increased their activity levels after knee replacement surgery (12).
Unrealistic expectations about knee replacement surgery only increase dissatisfaction with the results
Patients are often under the impression that knee replacement surgery will solve all the outstanding problems they’ve been experiencing with their knees. Unfortunately, the data does not support these kinds of expectations, leaving many patients dissatisfied with only mild changes post-surgery. As a matter of fact, many experts in the field are now questioning whether knee replacement surgery is being recommended and performed too often, or too soon, on patients who have not yet devoted adequate time to learn about alternative approaches to the surgery.
You owe it to yourself to understand the risks and results of knee replacement surgery, but also to be aware of other alternatives to the surgery that may end up providing similar or better results. Here are three alternatives to knee replacement surgery, other than the PKA:
Steroid injections
These injections, also known as corticosteroids or cortisone, are a common treatment for knee osteoarthritis. These steroids are potent anti-inflammatories, helping with bad inflammation that results in knee pain, but they are also not without risk. Some high-level research has shown that steroid injections can destroy cartilage, and aren’t as effective as they once were thought to be (13). These should not be considered a viable long-term treatment option for patients with knee arthritis.
Viscosupplementation
This process is also a highly common treatment for knee osteoarthritis. Viscosupplementation involves gel shots into the knee, also known as hyaluronic acid. There has been no research that indicates that viscosupplementation harms cartilage in the same way that steroid injections can, and much research supports the benefit of hyaluronic acid for arthritis pain. However, studies have returned mixed reviews on the long-term effectiveness of viscosupplementation, with some research providing positive effect data, and other research indicating no real, lasting change (14,15).
Knee Nerve Ablation
One of the most recent trends in alternative treatments for knee replacement is knee nerve ablation, or ablating the pain nerves centered around the knee. This technology involves the doctor placing probes close to several nerves surrounding the joint, using electrical energy to destroy, or ablate, them. These are the nerves that take pain signals from the knee to the brain, so by ablating the nerves, the pain goes away until the nerves grow back. Research proving this method’s effectiveness is still limited (17,18) because the procedure is still in the early stages of use; no high-level studies have been conducted on this particular treatment method at this point.
At Centeno-Schultz, we perform this leading, innovative procedure as a treatment for knee osteoarthritis in efforts to reduce knee pain and improve overall function. Our treatments are backed by extensive research and published patient outcome data, and all of our doctors are musculoskeletal specialists with advanced training.
Our preferred Treatment for AC Joint Impingement is PRP for
Outcomes
Knee Function Improvement After Regenexx Procedure
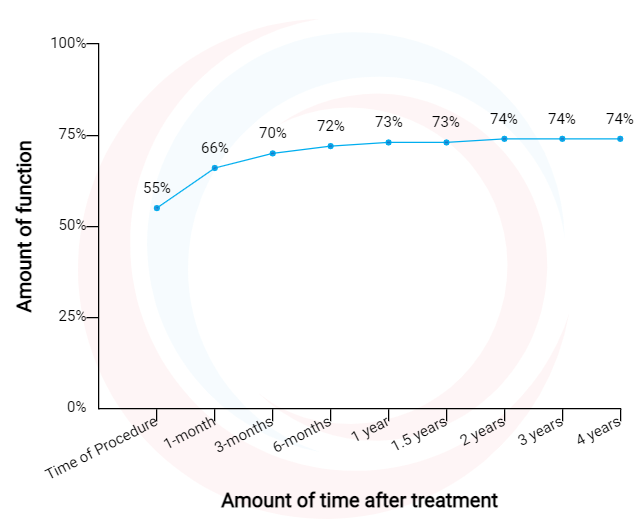
Data updated March 01, 2021.
Knee Pain Decrease After Regenexx Procedure
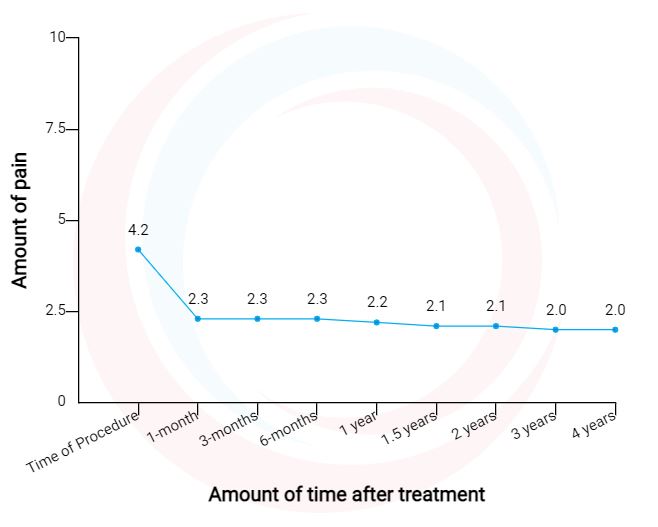
Data updated March 01, 2021.
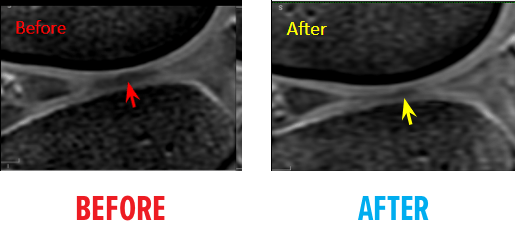
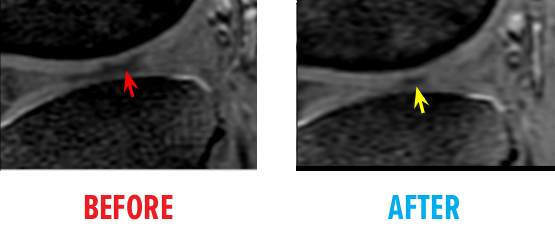
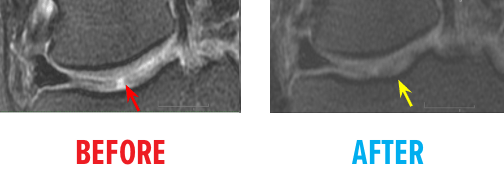
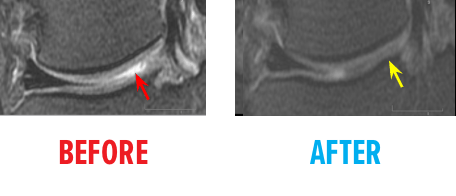
Before & After MRI
46-year-old white female status post an unsuccessful arthroscopic debridement where a large 3cm by 4 cm osteochondral defect on the medial femur was discovered. She underwent Regenexx ACL tear treatment at 1.5 years after surgery and returned to full functioning.
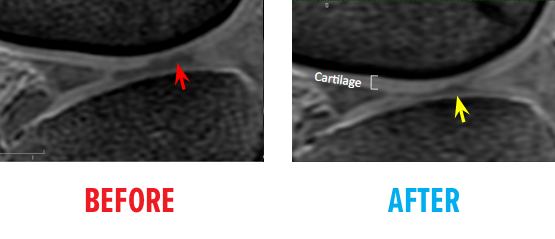
51-year-old white female status post unsuccessful micro-fracture for large osteochondral defect. Patient was unable to return to many activities after micro-fracture and as a result, underwent percutaneous, autologous, mesenchymal stem cell implant. She returned to full activities with this knee.

References
(1) Medical Advisory Secretariat. Total knee replacement: an evidence-based analysis. Ont Health Technol Assess Ser. 2005;5(9):1–51. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3382388/
(2) Sakellariou VI, Poultsides LA, Ma Y, Bae J, Liu S, Sculco TP. Risk Assessment for Chronic Pain and Patient Satisfaction After Total Knee Arthroplasty. Orthopedics. 2016 Jan-Feb;39(1):55-62. doi: 10.3928/01477447-20151228-06.
(3) Wylde V, Hewlett S, Learmonth ID, Dieppe P. Persistent pain after joint replacement: prevalence, sensory qualities, and postoperative determinants. Pain. 2011 Mar;152(3):566-72. doi: 10.1016/j.pain.2010.11.023.
(4) Friesenbichler J, Maurer-Ertl W, Sadoghi P, Lovse T, Windhager R, Leithner A. Serum metal ion levels after rotating-hinge knee arthroplasty: comparison between a standard device and a megaprosthesis. Int Orthop. 2012;36(3):539–544. doi: 10.1007/s00264-011-1317-4
(5) Savarino L, Tigani D, Greco M, Baldini N, Giunti A. The potential role of metal ion release as a marker of loosening in patients with total knee replacement: a cohort study. J Bone Joint Surg Br. 2010 May;92(5):634-8. doi: 10.1302/0301-620X.92B5.23452.
(6) Savarino L, Tigani D, Greco M, Baldini N, Giunti A. The potential role of metal ion release as a marker of loosening in patients with total knee replacement: a cohort study. J Bone Joint Surg Br. 2010 May;92(5):634-8. doi: 10.1302/0301-620X.92B5.23452.
(7) Atanaskova Mesinkovska N, Tellez A, Molina L, Honari G, Sood A, Barsoum W, Taylor JS. The effect of patch testing on surgical practices and outcomes in orthopedic patients with metal implants. Arch Dermatol. 2012 Jun;148(6):687-93. doi: 10.1001/archdermatol.2011.2561.
(8) Hinarejos P, Ferrer T, Leal J, Torres-Claramunt R, Sánchez-Soler J, Monllau JC. Patient-reported allergies cause inferior outcomes after total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2016 Oct;24(10):3242-3246. https://www.ncbi.nlm.nih.gov/pubmed/26531183
(9) Belmont PJ Jr1 Goodman GP, Kusnezov NA, Magee C, Bader JO, Waterman BR, Schoenfeld AJ. Postoperative myocardial infarction and cardiac arrest following primary total knee and hip arthroplasty: rates, risk factors, and time of occurrence. J Bone Joint Surg Am. 2014 Dec 17;96(24):2025-31. doi: 10.2106/JBJS.N.00153.
(10) Waterman BR, Belmont PJ Jr, Bader JO, Schoenfeld AJ. The Total Joint Arthroplasty Cardiac Risk Index for Predicting Perioperative Myocardial Infarction and Cardiac Arrest After Primary Total Knee and Hip Arthroplasty. J Arthroplasty. 2016 Jun;31(6):1170-1174. doi: 10.1016/j.arth.2015.12.013.
(11) Kahn TL, Schwarzkopf R. Does Total Knee Arthroplasty Affect Physical Activity Levels? Data from the Osteoarthritis Initiative. J Arthroplasty. 2015 Sep;30(9):1521-5. doi: 10.1016/j.arth.2015.03.016
(12) Harding P, Holland AE, Delany C, Hinman RS. Do activity levels increase after total hip and knee arthroplasty? Clin Orthop Relat Res. 2014 May;472(5):1502-11. doi: 10.1007/s11999-013-3427-3.
(13) McAlindon TE, LaValley MP, Harvey WF, et al. Effect of Intra-articular steroid vs Saline on Knee Cartilage Volume and Pain in Patients With Knee Osteoarthritis: A Randomized Clinical Trial. JAMA.2017;317(19):1967–1975. doi: 10.1001/jama.2017.5283
(14) Rutjes AW, Jüni P, da Costa BR, et al. Viscosupplementation for Osteoarthritis of the Knee: A Systematic Review and Meta-analysis. Ann Intern Med. 2012;157:180–191. doi: 10.7326/0003-4819-157-3-201208070-00473
(15) Strand V, McIntyre LF, Beach WR, Miller LE, Block JE. Safety and efficacy of US-approved viscosupplements for knee osteoarthritis: a systematic review and meta-analysis of randomized, saline-controlled trials. J Pain Res. 2015;8:217–228. Published 2015 May 7. doi:10.2147/JPR.S83076
(16) Altman RD, Dasa V, Takeuchi J. Review of the Mechanism of Action for HA in Knee Osteoarthritis. Cartilage. 2018;9(1):11–20. doi:10.1177/1947603516684588
(17) El-Hakeim EH, Elawamy A, Kamel EZ, Goma SH, Gamal RM, Ghandour AM, Osman AM, Morsy KM. Fluoroscopic Guided Radiofrequency of Genicular Nerves for Pain Alleviation in Chronic Knee Osteoarthritis: A Single-Blind Randomized Controlled Trial. Pain Physician. 2018 Mar;21(2):169-177. https://www.ncbi.nlm.nih.gov/pubmed/29565947
(18) Gupta A, Huettner DP, Dukewich M. Comparative Effectiveness Review of Cooled Versus Pulsed Radiofrequency Ablation for the Treatment of Knee Osteoarthritis: A Systematic Review. Pain Physician. 2017 Mar;20(3):155-171. https://www.ncbi.nlm.nih.gov/pubmed/28339430