The pain is debilitating. Medications and therapy have not helped. Your doctor believes you have a nerve injury. He is not certain of the next step. What is Nerve Hydrodissection? Which nerves can be treated with Hydrodissection? What causes nerve compression? What does nerve pain feel like? What is our history with nerve regeneration? How is Nerve Hydrodissection performed at the Centeno-Schultz Clinic? How does one prepare for the procedure? Let’s dig in.
What Is Nerve Hydrodissection?
Nerve Hydrodissection is a medical procedure that aims to free up scar tissue or adhesions on a given peripheral nerve (1). The procedure utilizes ultrasound guidance to visualize both the needle and the targeted nerve. Medication is then injected through the needle to free up the scar tissue. Nerve Hydrodissection is a minimally invasive treatment option for many peripheral nerves that are compressed or entrapped by scar tissue.
Which Nerves Can be Treated with Hydrodissection? (Median, Ulnar, LFC, Saphenous)
Compression, scar tissue formation, or irritation can affect virtually any nerve. Hydrodissection has been used in nerve injuries (2). The most common include:
Median Nerve
The Median nerve is an important nerve in the hand and wrist. It travels through a very narrow tunnel as it passes from the forearm to the hand. It is susceptible to injury. Irritation or compression of the Median nerve can result in carpal tunnel syndrome. Carpal tunnel syndrome is a common, painful medical condition that occurs as a result of irritation or compression of the Median nerve. Pain and numbness are common. Studies have shown hydrodissection to be effective in the treatment of patients with carpal tunnel syndrome.
J Smith demonstrated the procedure to be effective in reducing symptoms (3).
DeLea et al. performed a prospective study demonstrating a reduction in pain and improved blood flow with this approach (4).
Ulnar Nerve
Cubital Tunnel Syndrome is a common, painful medical condition in which the Ulnar nerve is compressed at the level of the elbow. Studies have demonstrated Nerve Hydrodissection to be effective in the treatment of patients with Cubital Tunnel Syndrome.
Kim et al. demonstrated that hydrodissection could separate the Ulnar nerve from the boney surface and the adjacent connective tissue (5).
Choi demonstrated similar success with a reduction in pain, reduced nerve swelling under ultrasound, and improvement in nerve testing results (6).
Lateral Femoral Cutaneous Nerve
The Lateral Femoral Cutaneous nerve when irritated or compressed can result in tingling, numbness, and burning pain in the outer part of your thigh. The syndrome is called Meralgia Paresthetica. Nerve Hydrodissection of the lateral cutaneous nerve in one study provided a complete resolution of all symptoms in all patients at 2 months post-injection (7)
Saphenous Nerve
Saphenous nerve irritation or injury can cause debilitating knee pain that is localized on the medial (inside) aspect of the knee. In a small clinical study, Clendenen demonstrated hydrodissection to be effective with 75% of patients noting a significant reduction in pain (8).
What Factors May Cause Nerve Compression (Trauma, Bone Spurs, Tendonitis, Surgery & Fracture)
There are a number of factors that put a patient at risk for nerve compression. The most common include:
Sports Injuries
Atheltic injuries are often times associated with significant bending, twisting, and torquing of an extremity. Nerves don’t fair well with abrupt, high-velocity stretching, bending, or twisting. The result can be nerve compression and pain.
Bone Spurs
Bone spurs are bony projections that develop along bone edges. They can vary in size and shape. Some are smooth whereas others are coarse with irregular edges They are composed of bone which can easily irritate or compress nerves. The result can be significant pain and often times numbness and weakness.
Tendonitis/ Tendinosis
Tendons are thick pieces of connective tissue that connect muscle to bone. Tendons are susceptible to injury which can cause inflammation and swelling of the tendon. This is called tendonitis. Tendons can also become degenerative which is called tendinosis. Both conditions can result in nerve compression and pain.
Post Surgery
Surgery is often associated with the formation of scar tissue. This scar tissue can irritate or compress a nerve as well as altering its normal course as it descends through the body.
Post Fracture
A fracture involves the breaking of a bone. There are different types which include simple, compound, incomplete and complete fractures. The trauma causing the fracture or the subsequent healing and formation of scar tissue can result in nerve irritation or compression.
Baxter’s Neuropathy
It is an entrapment syndrome, like carpal tunnel syndrome in your hand. This is an entrapment of a nerve in your foot, right around your heel, on the inside part compressing a branch of your tibial nerve called your inferior calcaneal nerve, and that is the Baxter’s nerve. Now, the inferior calcaneal nerve is the first branch of the lateral plantar nerve, which is a branch off your tibial nerve. It lives between a muscle belly called your abductor hallucis muscle, as well as the medial calcaneal tuberosity, which is a small bump where a common heel spur occurs in the foot.
Bone spurs, also known as osteophytes, are abnormal growths that can form along any bony surface in the body. They most frequently occur where tendons and ligaments attach to the bone. As a result, they are more commonly seen in large mobile joints that support weight, such as the hips, spine, ankles, or knees.
Surprisingly, most bone spurs are relatively benign but are a clinical sign of instability in the area. Research demonstrates that if a ligament has laxity, the constant strain at the insertion into the bone will elevate the surface of the bone, creating additional bone formation – this is known as a traction osteophyte.
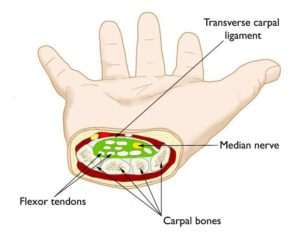
The carpal tunnel is a tunnel-like structure in the wrist that the median nerve travels through. There are also carpal ligaments that form the roof of the tunnel and flexor tendons that also run through the tunnel. The median nerve is a branch that generates off the brachial plexus from the cervical spine in the neck. It stretches down through the arm, the wrist, and all the way into the thumb. The flexor tendons provide stability and help bend the thumb and fingers. When something causes the tunnel to narrow or the medial nerve somehow becomes compressed in the wrist, this can lead to carpal tunnel syndrome (CTS).
Golfer’s elbow involves tears in the ulnar collateral ligament and pain or soreness on the inside of the elbow. The bony bump you feel there is the medial epicondyle of the humerus (upper arm bone). There are five forearm muscles that attach at this point, all of which are involved in helping to flex or rotate the forearm and wrist. Pain can get worse when you throw a ball, grip a dumbbell, turn a screwdriver, and other movements that involve the fingers, hand, wrist, and/or elbow. Tennis elbow is similar, however, it refers to the outside of the elbow, at the lateral epicondyle.
Guyon canal syndrome is a condition caused by the compression of the ulnar nerve as it passes through the Guyon canal, a narrow passageway located on the palm side of the wrist. This syndrome is commonly seen in people who perform repetitive tasks with their hands or use tools that vibrate, such as jackhammers or drills. Other causes of Guyon canal syndrome may include trauma or injury to the wrist, arthritis, or tumors. Treatment for Guyon canal syndrome may include immobilization of the wrist, anti-inflammatory medications, physical therapy, or– in severe cases– surgery. If left untreated, Guyon canal syndrome can lead to permanent nerve damage, muscle weakness, and loss of function in the affected hand and wrist.
The common peroneal nerve branches behind the knee and this could be irritated from any overuse activity, surgery, instability, or any compression on the outside of the knee. Typically, this will present as pain on the outside of the knee radiating towards the baby toe, the calf, and the lateral shin towards the lateral ankle. What Causes Peroneal Nerve Compression? There are many potential causes of peroneal nerve compression, such as overuse activities, surgery, instability, or any compression on the outside of the knee. Trauma and nerve compression, especially caused by a fractured or dislocated ankle, can all cause injury to the peroneal nerve. Causes include:
We talk a lot about leg pain stemming from a pinched or irritated nerve in the lower back. And, indeed, that’s what our physicians are traditionally taught in medical school—a pinched nerve in the lumbar spine typically presents as a symptom in the leg. However, what if you have some butt pain but no pain or other symptoms in the leg? Does this mean it couldn’t be a pinched nerve? Not so fast. Turns out a pinched low back nerve doesn’t always have to be accompanied by leg symptoms.
Let’s start by taking a look at how the back is structured.
Carpal tunnel syndrome is compression of the median nerve at the level of the wrist with resultant hand and wrist pain. Tarsal tunnel syndrome (TTS) is the equivalent in the ankle.
What is Tarsal Tunnel Syndrome (TTS)?
Also called tibial neuralgia, TTS is compression of the tibial nerve as it passes through the tarsal tunnel at the ankle. The tarsal tunnel is located behind the medial malleolus, the bump on the inside of the ankle.
Thoracic radiculopathy is a painful medical condition that affects both men and women alike. Pain, paresthesia, decreased sensation, and weakness are the major symptoms. Radiculopathy refers to the whole complex of symptoms that can be caused by irritation or compression of a nerve root in the spine. Thoracic radiculopathy is irritation or compression of a thoracic spinal nerve. Causes of radiculopathy in the thoracic region are thoracic disc injuries, thoracic facet arthritis, ligament thickening, facet cyst, unstable rib attachments, and bone spurs. Diagnosis of thoracic radiculopathy can be difficult….
Simply put, ulnar neuropathy refers to the compression or damage to the ulnar nerve in the arm. It affects up to 6% of the population, based on reports.The ulnar nerve is one of three main nerves in the arm that run from the shoulder to the hand and is responsible for providing sensation to the small and ring fingers and for controlling the movement of specific hand muscles. When the ulnar nerve is damaged or compressed, it can lead to a range of symptoms, including pain, numbness, weakness, and tingling in the affected hand. The symptoms of ulnar neuropathy can…
Pain is an uncomfortable and at times painful sensation. It varies significantly from patient to patient. There are many different types of pain which include inflammatory, nociceptive, and neuropathic. Neuropathic pain is pain that arises from nerve compression or injury. Nerve pain has the following characteristics (9).
Deep-seated pain
Poorly localized
Varying presentations that include soreness, numbness, pins, and needles, heaviness, or electrical shock
Nerve Regeneration at the Centeno-Schultz Clinic
Our history with the nerve regeneration procedure begins with a different form of PRP. Traditional PRP used by most clinics is very inflammatory and can actually aggravate nerves that are irritated or compressed. At the Centeno-Schultz Clinic, we have another type of PRP treatment called Platelet Lysate (PL). Platelet Lysate is not inflammatory and it works well with and around nerves. In 2007 we started using Platelet Lysate to treat patients with Sciatica with great results. This led to a publication where we demonstrated Platelet Lysate epidural injections were superior to traditional high dose steroid injections (citation). How does this happen? Platelet Lysate is rich in growth factors that can increase blood flow, reduce inflammation and promote healing. To learn more about the healing properties of Platelet Lysate please click on the video below.
Nerve Hydrodissection at Centeno-Schultz Clinic
Nerve Hydrodissection is not a painful procedure. It starts with you being comfortably positioned in a procedure room. Monitors are applied for your safety. The area is then washed with sterile soap. An ultrasound is used to clearly identify the affected nerve. Ultrasound, also called Sonography uses high-frequency sound waves to create an image of a specific body part. Nerve Hydrodissection is a procedure intended for peripheral nerves. What are those? They are nerves that have already exited the spine and are traveling down arm or leg to their final destination. Examples include the Median, Radial, and Saphenous nerves.
Different views of the targeted nerve are taken which include cross-section views and long-axis views. The size of the nerve as well as its different parts is carefully evaluated. In some cases, the nerve itself is swollen. In other cases, the fascicles within the nerve are swollen. This is illustrated below. On the left, the actual nerve is swollen as reflected in the increase in diameter of the nerve. On the right, the fascicle is swollen which is one of the bundles within the nerve. It takes extensive training to identify these findings under ultrasound.
The next step involves advancing a small needle under ultrasound towards the affected nerve. Hazards abound as one must avoid adjacent veins and arteries which are susceptible to injury. The nerve itself can also be further injured if traumatized by the needle. The needle is advanced until it is immediately adjacent but NOT in the nerve. Platelet Lysate is then very carefully and very slowly injected. The fluid and not the needle itself frees up the scar tissue and adhesions that are compressing the nerve. The procedure is performed in a circumferential fashion such that the entire surface of the nerve is coated with Platelet Lysate.
Outside of the mechanical effects of breaking up scar tissue, we believe the growth factors in PL can help nerve function. One of those natural compounds is called Vascular Endothelial Growth Factor or VEGF and is responsible for causing the body to create new blood vessels. Nerves have a blood supply like any other tissue and much of that lives on the outside of the nerve. When nerves have pressure placed on them, that blood supply can be cut off, reducing oxygen to the nerve. So creating new blood vessels around nerves may be important in nerve regeneration.
This is a technically challenging procedure that your PCP or orthopedic surgeon can not perform. To watch a Median Nerve Hydrodissection please click on the video below.
A Clinical Success Story: Meet MS
At the Centeno-Schultz Clinic, we are experts in the diagnosis and treatment of nerve pain. Utilizing Nerve Hydrodissection with a patient’s own platelets we have helped a large number of patients with nerve compression problems. The most common involves Carpal Tunnel Syndrome which involves compression of the Median Nerve. To learn more about Carpal Tunnel Syndrome please click here. Other clinical compression conditions have also been successfully treated.
MS is a 57 y/o patient who injured his left Humerus ( upper arm bone) after falling from a ladder. He also injured the Radial Nerve (the nerve that gives a signal to the muscle that causes wrist extension and sensation to the back of the hand). He had surgery to repair the humeral fracture, but the Radial Nerve was severely injured so he was left with “Radial Nerve Palsy.” This is where the muscles that the radial nerve supplied no longer worked well. This was tragic!
Why? Because he was unable to move his fingers and wrist in extension and had numbness and burning pain in the back of the hand. The surgeon offered no physical therapy and informed him that it was unlikely that he would return to playing golf, one of his life long passions. Nerve conduction studies showed a damaged Radial Nerve. Dr. Pitts provided MS with hope as he knew the potential of Nerve Hydrodissection. 6 weeks after the tragic fall from the ladder, MS underwent Nerve Hydrodissection with his own platelets. Within 2 weeks of the first procedure, he began noticing an increase in finger movement. He ultimately received 4 treatments over 6 months and below is his update at 9 months after his initial injury:
“I do not believe my recovery is a miracle! I am convinced it is the result of sound medical science and skilled treatment. My orthopedic surgeon and neurologist gave me little chance of resuming playing golf, due to my radial nerve palsy, emanating from a fractured left humerus. The surgery to repair this injury required 9 screws and a plate. My drooping left wrist and lack of any sort of fine motor skills with my hand were evidence of that. Now, nine plus months after injury and seven plus months after beginning treatment, I now have 95% use of my wrist and 85%+ use of my hand. My key indicator with regard to re-establishing my coordination is my golf handicap. My handicap has grown from 3.8 to 4.9 and my low score post injury is 75 (twice), 3 over par. My best the previous year was even par 72 (twice). Golf is an extreme hand-eye coordination sport and I believe a good indicator of the level of recovery for my dexterity, strength and fine motor skills…I believe the nerve hydrodissection in four treatments has produced remarkable results. Progress has now slowed, but is still proceeding.”
How to Prepare for Nerve Hydrodissection? (Avoid NSAID, Steroids and Blood Thinners)
The following medications should be avoided:
NSAID’s
NSAID’s such as Motrin, Aleve, and Voltaren can adversely affect your platelets and clinical outcome.
Steroids
Steroids are powerful anti-inflammatory agents but have significant toxic effects including cartilage, tendon, and ligament injuries. To learn more about the adverse effects of steroids please click here.
Blood Thinners
Blood thinners can increase the risk of post-procedure bleeding which can compromise nerve well being and healing.
Tobacco should also be avoided as it can significantly reduce the blood to a given area. Remember blood flow is essential for healing and reduction of inflammation
In Conclusion
Peripheral nerves are those nerves that have already exited the brain and spine and travel down into the arms and legs.
Peripheral nerves are susceptible to injury, irritation, compression, and entrapment.
Common examples of peripheral nerves include the Median, Ulnar and Saphenous nerves.
Carpal Tunnel Syndrome and Cubital Tunnel Syndrome are common clinical conditions that involve peripheral nerve compression and pain.
Nerve Hydrodissection is a minimally invasive medical procedure that aims to free up the scar tissue or adhesions that are irritating or compressing a given peripheral nerve.
Nerves that have been successfully treated with hydrodissection include the Median, Ulnar, Lateral Femoral Cutaneous and Saphenous nerves.
Factors that may cause nerve compression include trauma, bone spurs, tendonitis, surgery, and fractures
Nerve pain is deep-seated, poorly localized, and may include numbness and or the sensation of pins and needles.
The Centeno-Schultz Clinic has an extensive history of nerve regeneration procedures involving a specialized PRP called Platelet Lysate.
During a Nerve Hydrodissection procedure, the scar tissue or adhesions around a targeted nerve is mechanically released using Platelet Lysate and a local anesthetic that is injected through a small gauge needle. The pressure exerted by the injected fluid mechanically releases the scar tissue thereby relieving the compression on the nerve. The growth factors from the PRP reduce inflammation and increase blood flow thereby promoting healing.
The procedure is easy and requires that NSAIDs, steroids, and blood thinners be avoided prior to the procedure.
If you or a loved one suffer from ongoing nerve pain due to compression or entrapment please schedule a telemedicine consultation. Alternatively, if you live in the greater Denver-Boulder area schedule an in-office evaluation and have a diagnostic ultrasound. Have a board-certified, fellowship-trained physician review your history and discuss possible regenerative treatment options. Living with the pain or masking it with medications are not your only options. Call or schedule today before the injury progresses leading to more pain and limitation.
Doctors Who Use Nerve Hydrodissection at Centeno-Schultz Clinic
Christopher J. Centeno, MD
Christopher J. Centeno, M.D. is an international expert and specialist in Interventional Orthopedics and the clinical use of bone marrow concentrate in orthopedics. He is board-certified in physical medicine and rehabilitation with a subspecialty of pain medicine through The American Board of Physical Medicine and Rehabilitation. Dr. Centeno is one of the few physicians in the world with extensive experience in the culture expansion of and clinical use of adult bone marrow concentrate to treat orthopedic injuries. His clinic incorporates a variety of revolutionary pain management techniques to bring its broad patient base relief and results. Dr. Centeno treats patients from all over the US who…
John R. Schultz M.D. is a national expert and specialist in Interventional Orthopedics and the clinical use of bone marrow concentrate for orthopedic injuries. He is board certified in Anesthesiology and Pain Medicine and underwent fellowship training in both. Dr. Schultz has extensive experience with same day as well as culture expanded bone marrow concentrate and sees patients at the CSC Broomfield, Colorado Clinic, as well the Regenexx Clinic in Grand Cayman. Dr. Schultz emphasis is on the evaluation and treatment of thoracic and cervical disc, facet, nerve, and ligament injuries including the non-surgical treatment of Craniocervical instability (CCI). Dr. Schultz trained at George Washington School of…
Dr. Pitts is originally from Chicago, IL but is a medical graduate of Vanderbilt School of Medicine in Nashville, TN. After Vanderbilt, he completed a residency in Physical Medicine and Rehabilitation (PM&R) at Emory University in Atlanta, GA. The focus of PM&R is the restoration of function and quality of life. In residency, he gained much experience in musculoskeletal medicine, rehabilitation, spine, and sports medicine along with some regenerative medicine. He also gained significant experience in fluoroscopically guided spinal procedures and peripheral injections. However, Dr. Pitts wanted to broaden his skills and treatment options beyond the current typical standards of care.
Post-residency, Dr. Markle was selected to the Interventional Orthopedic Fellowship program at the Centeno-Schultz Clinic. During his fellowship, he gained significant experience in the new field of Interventional Orthopedics and regenerative medicine, honing his skills in advanced injection techniques into the spine and joints treating patients with autologous, bone marrow concentrate and platelet solutions. Dr. Markle then accepted a full-time attending physician position at the Centeno-Schultz Clinic, where he both treats patients and trains Interventional Orthopedics fellows. Dr. Markle is an active member of the Interventional Orthopedic Foundation and serves as a course instructor, where he trains physicians from around the world.
Dr. Money is an Indiana native who now proudly calls Colorado home. He attended medical school at Kansas City University and then returned to Indiana to complete a Physical Medicine and Rehabilitation residency program at Indiana University, where he was trained on non-surgical methods to improve health and function as well as rehabilitative care following trauma, stroke, spinal cord injury, brain injury, etc. Dr. Money has been following the ideology behind Centeno-Schultz Clinic and Regenexx since he was in medical school, as he believed there had to be a better way to care for patients than the status quo. The human body has incredible healing capabilities…
1.Lam KHS, Hung CY, Chiang YP, et al. Ultrasound-Guided Nerve Hydrodissection for Pain Management: Rationale, Methods, Current Literature, and Theoretical Mechanisms. J Pain Res. 2020;13:1957-1968. Published 2020 Aug 4. doi:10.2147/JPR.S247208
2.Cass SP. Ultrasound-Guided Nerve Hydrodissection: What is it? A Review of the Literature. Curr Sports Med Rep. 2016 Jan-Feb;15(1):20-2. doi: 10.1249/JSR.0000000000000226. PMID: 26745165.
3.Smith J, Wisniewski SJ, Finoff JT, Payne JM. Sonographically guided carpal tunnel injections, the ulnar approach. J. Ultrasound Med. 2008; 27: 1485–90.
7.Tagliafico A, Serafini G, Lacelli F, et al. Ultrasound-guided treatment of meralgia paresthetica (lateral femoral cutaneous neuropathy): technical description and results of treatment in 20 consecutive patients. J. Ultrasound Med. 2011; 30: 1341–6.
9. Finnerup NB, Haroutounian S, Kamerman P, Baron R, Bennett DLH, Bouhassira D, Cruccu G, Freeman R, Hansson P, Nurmikko T, Raja SN, Rice ASC, Serra J, Smith BH, Treede RD, Jensen TS. Neuropathic pain: an updated grading system for research and clinical practice. Pain. 2016 Aug;157(8):1599-1606. doi: 10.1097/j.pain.0000000000000492. PMID: 27115670; PMCID: PMC4949003.
Am I a Candidate?
To answer this question, fill out the candidate form below to request a new patient evaluation, and a patient advocate will reach out to you to determine your next steps. Your one-hour, in-office or telemedicine evaluation will be with one of the world’s experts in the field of Interventional Orthopedics.