A Short Story About Testicle Pain
DS is a 40 y/o patient with a 7-month history of right testicle pain which is constant in duration, 5/10 in severity, progressive in nature, throbbing in character and principally localized in the right testicle with intermittent radiations into the groin, anterior thigh and third right toe. The patient denies any traumatic injury. Treatment to date had included antibiotics, MRI, ultrasound evaluation of the testicle, ultrasound of the inguinal area to rule out hernia and anesthetic block performed by the urologist which provided 3 hours of pain relief. All studies were normal. The patient underwent surgical removal of the appendage of the testicle (epididymis) with no reduction in pain. The patient has a 3-year history of intermittent lower back and right leg pain.
The Exam
Physical examination was most significant for an abnormal neurologic and musculoskeletal examination. Specifically, the patient had decreased sensation to light touch and temperature along the right big toe and lateral aspect of right foot, profound muscle banding with multiple trigger points in the lower back and most importantly along the inner right thigh.
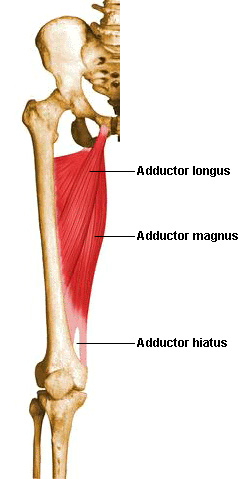
A thin gauge needle was inserted in the adductor Magnus at the most tender trigger point. This simple therapy provided DS with a 40% reduction in his testicular pain.
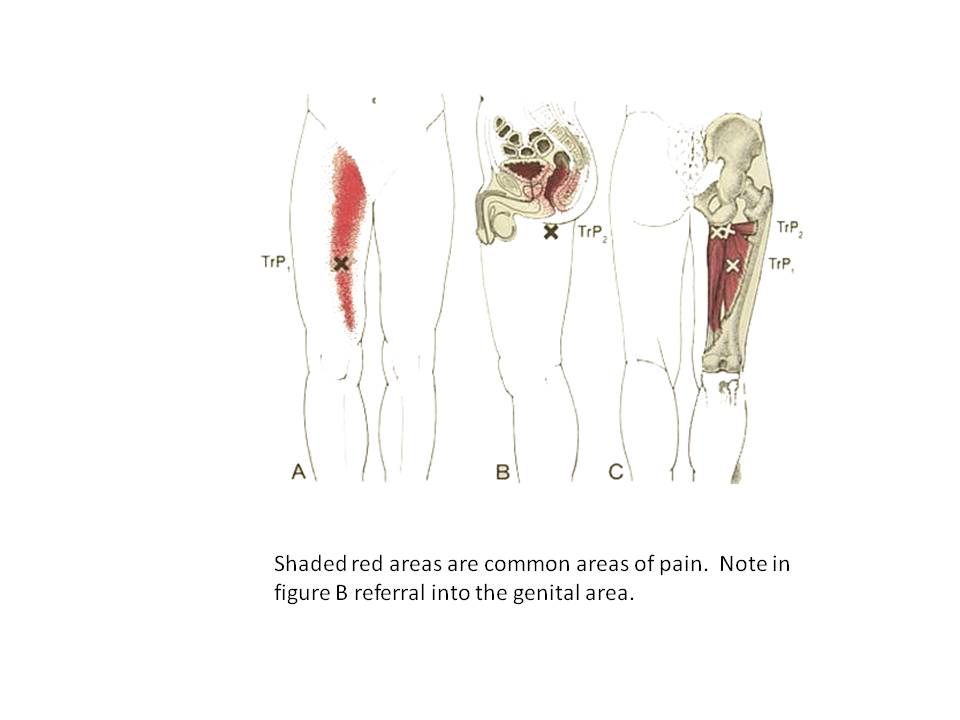
DS has a classic example of myofascial pain syndrome. A dysfunctional muscle caused referred pain. In DS’s case, his adductor Magnus was responsible for some of his testicular pain. He has just started therapy. He may also have some referred pain from the lumbar disc.
The adductor Magnus is a large fan-like muscle that attaches to the pelvis and femur. Its referral pattern is typically into the groin and testicle. There are other muscles with similar referral patterns.