The pain at the base of your skull is getting worse. It started gradually and now has gotten worse. Rest, massage, Motrin, and physical therapy has not helped. It is beginning to erode the quality of your life. Your PCP wants to start migraine medication, but the list of side effects is scary. Your chiropractor thinks the pain is arising from your upper neck. What is the Atlas bone? What is the Occiput? What is the Atlanto-Occipitial Joint? What are the key components of the AO Joint? What is the function of the AO Joint? Why is the Craniocervical Junction important? What are they major types of injuries to the AO Joint?
What Is the Atlas Bone?
The Atlas bone, also known as the C1 is the first bone in your neck (1). It is named after the Greek God Atlas who held up the world on his shoulders. The Atlas plays an important role as your skull rests directly on this bone.
What Is the Occiput?
The Occiput is the back portion of your skull. Otherwise known as your noggin. It provides important protection for your brain. At the base of the Occiput is a large opening called the Foramen Magnum. Foramen in Latin means opening. Magnum means large. So the Foramen Magnum is a large boney opening at the base of the skull which allows important structure to pass through (2).
The two most important structures are:
Spinal Cord
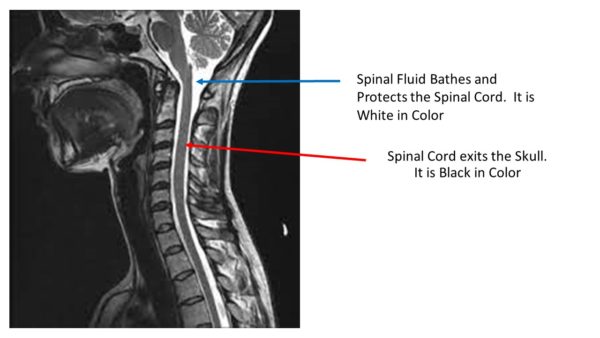
The Spinal Cord consists of neural tissue that starts at the base of the brain and extends down into the low back. It is a cylindrical bundle of nerve fibers that control our voluntary and involuntary bodily functions. It carries signals between the brain and the rest of the body. As the Spinal Cord descends from the skull and through the neck and rest of the body it is protected by the spinal bones. The C1 bone, AKA the Atlas, C2 bone, AKA the Axis and all the other bones of the spine provide a boney armour to protect against injury. The Spinal Cord has an additional layer of protection afforded by the spinal fluid. The spinal fluid is also known as Cerebral Spinal fluid. It surrounds the Spinal Cord and extends the entire length of the spine. The image to the left is a side view of the head, neck and Spinal Cord. The Spinal Cord is black in color and exits the head through the foramen magnum. The white that surrounds the Spinal Cord is the spinal fluid. The spinal fluid provides an important layer of protection for the spinal cord.
Cranial Nerves
As the Spinal Cord descends through the Foramen Magnum and spine, important nerves branch off traveling to different parts of the body. There are a large number of nerves. These include the twelve Cranial nerves some of which control muscles whereas others are connected to internal organs such as the heart and lungs.
What Is the Atlanto-Occipitial Joint (AKA C0-C1 Joint)
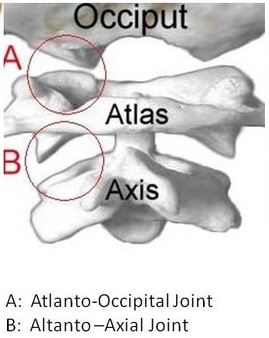
The Atlanto-Occipital Joint (AO) is a paired joint between the base of the skull and the cervical spine. The Occiput is numbered as C0 whereas the Atlas is numbered C1. Hence the Atlanto-occipital joint (AO) is the union of the C1 and C0 bones. Together they come together to form a joint that has as unique shape. It is saddle shaped joint as the convex surface of the Occiput fit into the concave surfaces of the C1 bone. The is a right and left AO Joint both of which are susceptible to injury.
The AO Joint is uppermost joint in the Cervical Spine. It is not be confused with the Atlanto-Axial (AA) Joint which is the C1/2 joint. To learn more about this joint please click here.
What Are the Key Components of the AO Joint? (Cartilage, Capsule, Ligaments & Muscles)
Cartilage
Like the knee joint, the AO Joint is lined with cartilage. Cartilage is the white shiny surface on the end of a bone that enables the smooth, pain-free movement of the joint. It absorbs and distributes large compressive and shear forces. The AO Joint is susceptible to injury and degeneration resulting in pain and reduced range of motion.
Capsule
The AA Joint has a capsule that covers the entire joint, It is a saran wrap-like covering composed of fibrous connective tissue. It provides support, distributes the forces, and limits the range of motion.
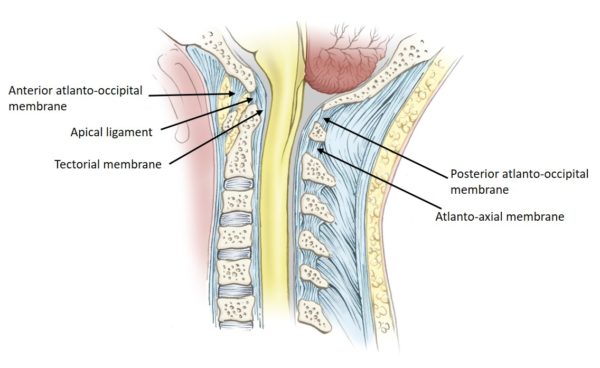
Ligaments
Anterior Atlantooccipital Ligament: Extends from the Foramen Magnum (hole in occiput) to the front of the C1 bone.
Posterior Atlantoocipital Ligament: Extends from the back of the Foramen Magnum to the back side of the C1 bone. It is a continuation of the Ligamentum Flavum.
Muscles
The are a large number of small muscles in the upper neck. They provide important support, stability and enable motion such as bending forward, backwards and rotating. One of the muscles called the Rectus Capitus Posterior Minor (RCPM) plays a very important role. It actually connects to the covering of the brain (3). It is called the Myodural Bridge. Clinically physicians have found that a tight or dyfucntional Rectus Capitus Posterior Minor muscle can put pressure on the Dura resulting in severe headaches
What Is the Function of the Atlanto-Occipital Joint? (Flexion & Extension)
The prinipcal function is bending forwards and backwards. This is referrred to as flexion and extension. An example is the movement made when nodding ” yes”.
The Atlantoaxial (AA) Joint is also part of the Craniocervical Junction. The Craniocervical Junction is the area between the Skull and the Cervical Spine (4). It consists of the bone that forms the base of the Skull, the first two bones in the Spine, and the neural structures that pass from the brain down into the Cervical Spine.
Why Is the Craniocervical Junction Important?
The Spinal Cord transmits essential information from the Brain into the body. The Spinal Cord is extremely fragile and is suspectible to trauma, compression and irritation. If the Altanto-Occiptial (AO) Joint is injured, unstable or degenerative the Spinal Cord and its transmitted information is at risk. The Craniocervical Junction which includes the AO Joint is a potential choke point for the information required for life itself. Symptoms will vary depending upon the severity of the injury or instability. This and much more will be discussed in the next blog.
What Are the Different Types of Injuries to Atlanto-Occipital Joint? (Arthritis, Fx, Instability, Dislocation)
There are several different types of injuries to the Atlanto-Occipital (AO) Joint. The most common include:
Osteoarthritis
The AO Joint is lined with cartilage that allows for smooth, pain free motion. Arthritis is a medical condition whereby this lining is eroded leading to pain, inflammation and reduced range of motion. Different conditions can lead to arthritis in the AO Joint which include: trauma, ASD and ligamental laxity.
Trauma
Winter and summer sports, martial arts and motor vehcile accidents can all potentially injure the AO Joint leading arthritic changes, pain and limited range of motion.
Adjacent Segment Disease (ASD)
ASD is a common phenomenon that occurs with neck surgery. The discs in the spine function to absorb the forces of daily living. Surgical fusion removes one or more discs compromising the biomechanics of the spine. Greater forces are then placed on the disc and joints above and below the fusion. These additional forces result in injury, degeneration and pain in the adjacent segements. We have seen numerous patients who have developed arthritis of the AO Joint due to prior neck surgery.
Ligament Laxity
Ligaments are thick pieces of connective tissue that connect bone to bone. When injured, stretched or torn they compromise the stability of a given joint. Micromotion of the joint can occur that leds to injury of the cartilage and joint capsule leading to pain, degneration and restriction in motion. Alar, Transverse, Anterior Longitudinal, X, Y ligament laxity can led to AO Joint degeneration and arthritis.
Fracture
The C1 bone can be bruised or fractured. A Jefferson fracture is fracture of the front or back aches of the C1 vertebra. The base of the skull AKA the Occiput can be bruised or fractured. Occiput fractures can be on one side (unilateral) or both sides (bilateral).
Dislocation
AO dislocation is most common in children and young adults. It is typically associated with high impact trauma such as motor-vehicle accidents or falls from heights (5). Dislocation occurs as a result of an injury to the upper neck ligaments. These include the Alar and Transverse ligaments. In severe cases the Spinal Cord is injured as it is choked and injured when passing from the skull into the neck. 70% of cases are fatal.
In Conclusion
The Atlas bone, also known as the C1 is the first bone in the Cervical Spine.
The Occiput is the back portion of the Skull. It is numbered as C0.
The Foramen Magnum is a large opening at the base of the Occiput. The Spinal Cord and Cranial Nerves exit the Skull through the Foramen Magnum.
The Atlanto-Occipital Joint (AO) is formed by the union of the Skull (C0) and the C1 bone.
The Atlanto-Occipital Joint is also known as the C0-C1 joint
The Atlanto-Occipital Joint (AO) is composed of cartilage, ligaments, muscles and tendons.
The principal function of the Atlantoaxial Joint is rotation.
The AA Joint is also part of the Craniocervical Junction.
The major types of injuries to the AO Joint are:
Osteoarthitis
Instability
Fracture
Dislocation
If you or a loved one has sustained an injury with ongoing headaches, neck pain, and dizziness that has not responded to conservative care please schedule a telephone candidacy discussion with a board-certified, fellowship-trained physician. At the Centeno-Schultz Clinic we are experts in the treatment of Atlanto-Occipit Injuries. From the comfort of your home or office learn what treatment options are available for you. Call today and stop the pain, misery, and suffering.
Could Craniocervical Instability Be the Cause of Your Symptoms?
Step 1
Imaging-Get movement based imaging
(DMX or Upright MRI with flexion and extension).
Step 2
Get Typed via a Telemed Appointment-There are 8 different types of CCI based on which
ligaments are Injured.
Step 3
Exam-If you’re a candidate for precise orthobiologic injections, you fly in for an exam and
treatment. A hands-on exam refines what we need to treat.
Step 4
Treatment-Get treated with a CCI focused, orthobiologic treatment plan tailored to you. That
includes PICL or whichever image guided, precise injections are the most likely to help you.
3.Zheng N, Chung BS, Li YL, Liu TY, Zhang LX, Ge YY, Wang NX, Zhang ZH, Cai L, Chi YY, Zhang JF, Samuel OC, Yu SB, Sui HJ. The myodural bridge complex defined as a new functional structure. Surg Radiol Anat. 2020 Feb;42(2):143-153. doi: 10.1007/s00276-019-02340-6. Epub 2019 Sep 28. PMID: 31563971.
5.Labler L, Eid K, Platz A, Trentz O, Kossmann T. Atlanto-occipital dislocation: four case reports of survival in adults and review of the literature. Eur Spine J. 2004 Mar;13(2):172-80. doi: 10.1007/s00586-003-0653-5. Epub 2003 Dec 13. PMID: 14673716; PMCID: PMC3476575.
6.Labler L, Eid K, Platz A, Trentz O, Kossmann T. Atlanto-occipital dislocation: four case reports of survival in adults and review of the literature. Eur Spine J. 2004 Mar;13(2):172-80. doi: 10.1007/s00586-003-0653-5. Epub 2003 Dec 13. PMID: 14673716; PMCID: PMC3476575.