
Cyclist Syndrome: What is it and how do we treat it?
Our clinic is situated between Boulder and Denver in Colorado, and both Boulder and Denver have a large cycling population! With that being said, we often evaluate patients with Cyclist Syndrome, also known as Pudendal neuralgia (or Pudendal Nerve Entrapment). This can be quite debilitating and traditional treatment options being limited, we have created a great way to allow cyclists to continue doing what they love, pain-free and without the need for medications or surgery! How? Let’s dig into this condition:
The Pudendal nerve (nerve that causes cyclist syndrome) is a combination of 3 nerves that form a single nerve. The sacral roots of S2, S3 and S4 exit the sacrum and then come together to form the Pudendal nerve in the periphery. Once formed, the 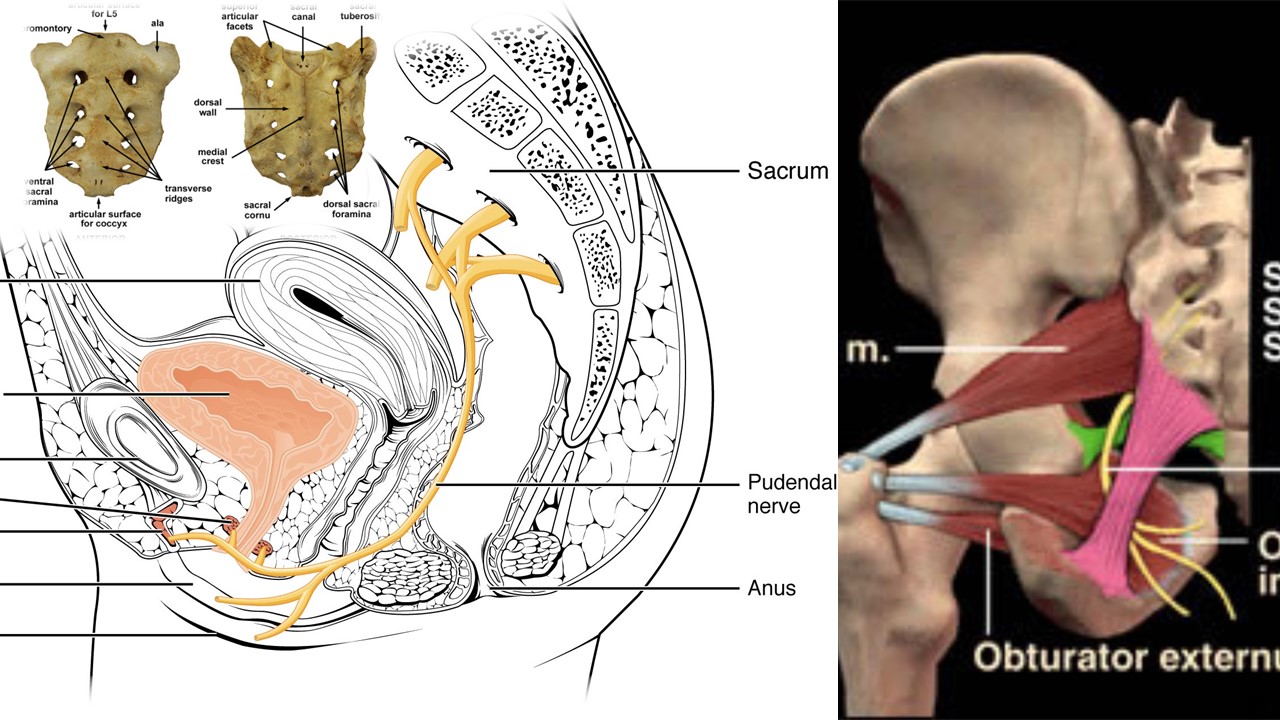
What causes Pudendal nerve entrapment?
The typical symptoms of Pudendal neuralgia in male competitive cyclists (it is often called “cyclist syndrome), who can develop recurrent numbness of the penis and scrotum after prolonged cycling, or an altered sensation of ejaculation, with disturbance of micturition (urination) and reduced awareness of defecation. Nerve entrapment syndromes, presenting as genitalia numbness, are among the most common bicycling associated urogenital problems (4).
Prolonged sitting on bicycle seat can cause a compressive force through the soft tissue. Continued over a period of time this creates a repetitive stress injury to the nerve and eventually causes symptoms. Repetitive stress to a peripheral nerve, damages the outer coating of the nerve (myelin) and once the myelin has been damaged, the nerve starts becoming hypersensitive, resulting in the symptoms. This type of mechanism is similar to what happens in carpal tunnel syndrome and in the low back with sciatica! Sitting on a bike is typically the biggest trigger of symptoms and hence why it has been termed cyclist syndrome!
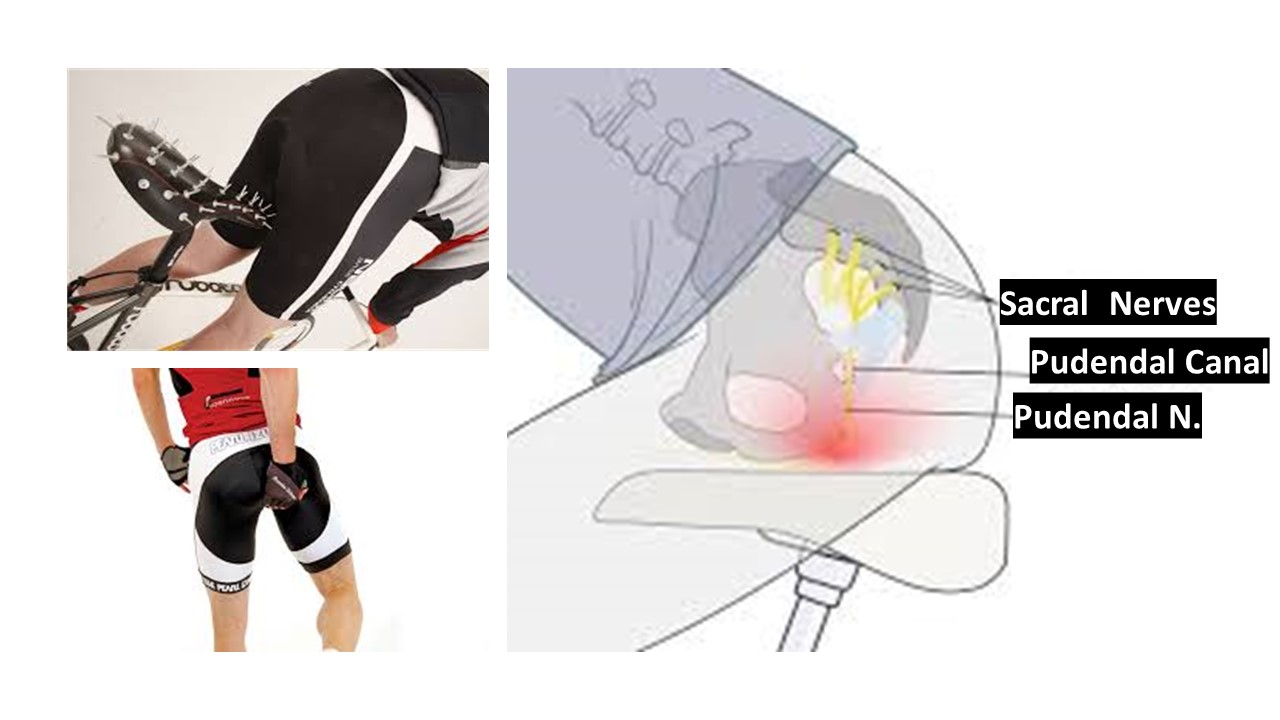
Genital numbness and erectile dysfunction are two of the major symptoms and the prevalence has been reported to be 50–91% and 13–24% respectively. The pain is typically caused by sitting, relieved by standing, and is absent when recumbent (lying down) or sitting on a toilet seat. If the perineal pain is positional (changes with the patient’s position, for example sitting or standing), this suggests a tunnel syndrome. Anesthesiologist John S. McDonald of UCLA reports that sitting pain relieved by standing or sitting on a toilet seat is the most reliable diagnostic parameter(5).
Other than positional pain and numbness, the main symptoms are fecal incontinence and urinary incontinence but this is less common compared to the pain and numbness.
How do you treat Pudendal nerve entrapment?
Initial treatment is (2-4):
- Ergodynamic evaluation to reduce the repetitive stress creating the damage. This can sometimes be going to a specialty bike shop to get properly fitted for a seat that can better reduce the stress to the nerve
- Physical therapy can also help strengthen the pelvic floor muscles as well as help relax tightened muscles.
- Medications: These are merely a pain reducer that can help decrease the severity of the symptoms. These can include anti-inflammatory medications (NSAIDS) or other drugs aimed neuropathic pain such as: anti-epileptics or antidepressants. These medications only mask the pain and unfortunately, do nothing to help the condition long-term.
- Corticosteroid injection: While this can give temporary reduction of symptoms, the likelihood of the pain returning is significant. In addition the negative local and systemic affects of high dose corticosteroids can be quite damaging.
- Radio-frequency ablation: Burning of the Pudendal nerve, like steroid injection, can be only temporary pain reduction. Side effects can be somewhat severe with post procedure pain, as possible motor loss creating weakness in the pelvic floor, erectile dysfunction, or loss of control to bowel and bladder function.
- Surgery: Surgical decompression of the Pudendal canal is considered a very last option!
New Treatment Option For Cyclist Syndrome / Pudendal Neuralgia
Being a leader in regenerative orthopedic medicine, we have successfully treated many cases of Pudendal Neuralgia by utilizing our 4th generation Platelet Lysate combined with precise ultrasound guided Pudendal Nerve hydro dissection! As mentioned above, the repetitive stress injury that created the nerve problem results in loss of myelin covering of the nerve. The concentration of immediate release growth factors help rebuild the myelin sheath thus resulting in healing of the nerve and reduction of symptoms! Here Dr. Centeno explains what Platelet Lysate is: https://regenexx.com/blog/whats-the-difference-between-prp-and-platelet-lysate/
Outside of PT and ergodynamic adjustments which are aimed at reducing the stress on the nerve, all other treatments are designed to treat the symptoms caused by the nerve injury BUT this new treatment option for Cyclist Syndrome / Pudendal Neuralgia is aimed at healing the nerve sheath and improving the electrophysiologic function of the nerve and thus reducing symptoms!
The Upside:
If you have or anyone you know has been dealing with cyclist syndrome or Pudendal neuralgia, please contact our office to set up an evaluation. Myself or one of my colleagues will discuss this advanced treatment option and your candidacy. If you have any questions, feel free to contact me via IG @ Dr.markle or through our patient care center.
References:
1. Khoder W, Hale D. Pudendal neuralgia. Obstet Gynecol Clin North Am. 2014;41(3):443‐452. doi:10.1016/j.ogc.2014.04.002
2. Pérez-López FR, Hita-Contreras F. Management of pudendal neuralgia. Climacteric. 2014;17(6):654‐656. doi:10.3109/13697137.2014.912263
3. Petrov-Kondratov V, Chhabra A, Jones S. Pulsed Radiofrequency Ablation of Pudendal Nerve for Treatment of a Case of Refractory Pelvic Pain. Pain Physician. 2017;20(3):E451‐E454.
4. Origo D, Tarantino AG. Osteopathic manipulative treatment in pudendal neuralgia: A case report. J Bodyw Mov Ther. 2019;23(2):247‐250. doi:10.1016/j.jbmt.2018.02.016
5. Ploteau S, Cardaillac C, Perrouin-Verbe MA, Riant T, Labat JJ. Pudendal Neuralgia Due to Pudendal Nerve Entrapment: Warning Signs Observed in Two Cases and Review of the Literature. Pain Physician. 2016;19(3):E449‐E454.
6. Tricard T, Munier P, Story F, Lang H, Saussine C. The drug-resistant pudendal neuralgia management: A systematic review. Neurourol Urodyn. 2019;38(1):13‐21. doi:10.1002/nau.23824
7. Gaines N, Odom BD, Killinger KA, Peters KM. Pudendal Neuromodulation as a Treatment for Persistent Genital Arousal Disorder-A Case Series. Female Pelvic Med Reconstr Surg. 2018;24(4):e1‐e5. doi:10.1097/SPV.0000000000000435