Understanding The Symptoms And Possible Causes Of A Frozen Shoulder
Are you experiencing pain and restricted range of motion in your shoulder? This pain may be due to a condition called adhesive capsulitis, more commonly known as frozen shoulder. Pain and restricted motion is a symptom of a frozen shoulder.
It is an inflammatory condition that affects the shoulder and causes restricted range of motion. In this post, we’ll discuss the symptoms of a frozen shoulder and its possible causes.
What Is A Frozen Shoulder?
Frozen shoulder, also known as adhesive capsulitis, is a painful loss of shoulder movement and range in motion. The incidence of frozen shoulder is 3-5% in the general population and up to 20% in those with diabetes (1). The peak incidence is between 40-60 years of age (2).
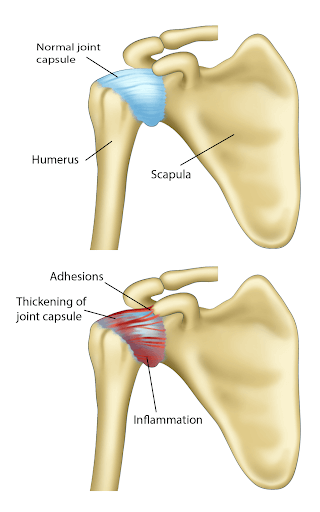
The exact mechanism is poorly understood. In general, the capsule becomes inflamed, thickened, and contracted, resulting in pain and a significant restriction in range of motion.
Causes Of Frozen Shoulder
The causes of frozen shoulder are poorly understood but may include trauma, prolonged immobility, systemic diseases such as diabetes, stroke, connective tissue disease, and heart disease. A frozen shoudler can also occur post-surgery and chronic inflammation which stimulates myofibroblasts to proliferate (3).
Symptoms
As the name suggests, frozen shoulder is a condition that results in loss of shoulder mobility – as if the shoulder is frozen – making it difficult to perform everyday activities.
A frozen shoulder has characteristic symptoms. These symptoms can wax and wane depending on the stage of the frozen shoulder. The following are some of the common symptoms of a frozen shoulder:
- Dull or aching pain in one shoulder: Unilateral shoulder pain is a common symptom of a frozen shoulder. This pain worsens over time across the different stages of a frozen shoulder.
- Worsening pain at night affecting the ability to sleep: Frozen shoulder pain is commonly worse at night when the patient is sleeping on their side. This position usually adds more pressure on the affected shoulder, aggravating any symptoms.
- Inability to move shoulder: Due to the increasing capsular stiffness, it can often become difficult to move the shoulder or complete any tasks within a normal range of motion. This limitation worsens gradually during the first two stages of a frozen shoulder.
The Three Stages Of A Frozen Shoulder
Frozen shoulder typically develops gradually in three phases: the freezing stage, the frozen stage, and the thawing stage. Each stage may last several months, and the symptoms may be slightly different in each stage.
- Freezing stage: The freezing stage is the initial phase of a frozen shoulder. During this stage, range of motion in the glenohumeral joint gradually becomes more and more restricted. Pain occurs when the arm is moved.
- Frozen stage: The frozen stage is the second stage of a frozen shoulder. The pain generally begins to lessen. However, the shoulder gets stiffer, making it more difficult to use.
- Thawing stage: The third stage is the thawing stage, also known as the recovery phase. During this stage, there is a gradual improvement in the range of motion and all other symptoms.
How Does One Get A Frozen Shoulder?
Frozen shoulders can occur through various mechanisms. They are explained briefly below:
- Thickening of shoulder capsule: The capsule of the shoulder joint thickens due to the deposition of scar tissue. This makes the capsule stiff and restricts any motion of the joint within.
- Shoulder immobility due to surgery or injury: If there is a history of injury or surgery, scar tissue or fibrous tissue may develop in the healing process. In addition, prolonged immobility following these incidences can further contribute to scar tissue, which may progress to a frozen shoulder.
- Natural degeneration: Degeneration of the tendons and the capsule can attract inflammatory cells. This can make the capsule stiff and lead to a frozen shoulder.
Possible Medical Conditions That May Cause A Frozen Shoulder
Certain medical conditions can increase the risk of developing a frozen shoulder. They are explained briefly below:
Diabetes
In diabetes, studies show that higher levels of glycated hemoglobin (HbA1c), advanced glycation end products (AGEs), vascular endothelial growth factor (VEGF), interleukin-1 beta (IL-1ß) can cause changes in the rotator cuff tendons and increase capsular stiffness (1). This can cause adhesive capsulitis.
Overactive Thyroid (Hyperthyroidism)
Hyperthyroidism is an autoimmune condition in which the thyroid is highly active. Graves’ disease is an overactive thyroid disorder that results in high amounts of interleukin-2 (IL-2), interferon-γ (IFN-γ), and tumor necrosis factor-α (TNF-α) cytokines being secreted by Th1 cells, causing the production of fibroblast cells (4).
These fibroblast cells lay down scar tissue which causes the joint capsule to stiffen, ultimately leading to a frozen shoulder.
Underactive Thyroid (Hypothyroidism)
Hypothyroidism can also lead to frozen shoulder. This is because the thyroid hormones are involved in the synthesis and degeneration of collagen (5). They also play a role in the proliferation and programmed self-death of human tenocytes.
Tenocytes are stretchy mechanosensitive tendon cells that make up the architecture of the tendon.
When the thyroid hormones are imbalanced due to an underactive thyroid, it can dysregulate the synthesis and cell death of tendon cells. This can cause them to degenerate which can lead to a frozen shoulder.
Hyperlipidemia
Low-density lipoprotein (LDL) cholesterol, known as the “bad cholesterol” in the medical space, is prone to oxidative modification. Oxidized LDL can induce endothelial cell activation in the walls of the blood vessel walls.
This attracts inflammatory cells and inflammation-related cytokines. These cytokines can stimulate the production of scar tissue which can lead to a frozen shoulder.
Tuberculosis
Tuberculosis can mimic the symptoms of and also cause a frozen shoulder. When tubercular mycobacteria infiltrate areas of high vascularity in the shoulder, a granuloma can develop. This is then followed by the destruction of the bone and surrounding tissues of the shoulder joint.
Bone-destroying cells and inflammatory cytokines are then released which further destroys the joint – sometimes even an abscess may form. As this heals, fibrous tissue may develop that can lead to a frozen shoulder.
In patients with a long-standing immobile shoulder and chronic shoulder pain that is worse at night, tuberculosis should be suspected.
Parkinson’s Disease
Parkinson’s disease can also increase the risk of a frozen shoulder. In this condition, posture is severely impaired due to increased thoracic kyphosis and decreased mobility of the trunk. This can cause subacromial impingement syndrome and capsulitis.
In turn, the bursa may become inflamed, reducing movement in the shoulder. With thoracic and shoulder motion affected, it can lead to a frozen shoulder. This becomes a vicious cycle as it can further worsen the posture, which worsens the impingement, and ultimately worsens the frozen shoulder symptoms.
Examination And Diagnosis
Your doctor will diagnose a frozen shoulder using the following steps:
- Physical examination: The doctor will examine your shoulder, neck, and upper back. The muscles and nerve supply of the shoulder joint will also be evaluated to see if there is any impingement or muscle tightness.
- Evaluation of active range of motion (ROM): The doctor will evaluate active ROM by asking you to move your arm and perform certain tasks against resistance.
- Evaluation of passive range of motion: The doctor will also evaluate the passive ROM of your shoulder by moving it while your shoulder is relaxed. These ROM tests will demonstrate the extent of the freeze in the shoulder and can also identify the stage of the frozen shoulder.
- Imaging: Initial X-rays are usually done to rule out other concomitant pathologies like fractures or dislocations. Additionally, an MRI can provide useful information about the rotator cuff and other muscles.
However, high-resolution musculoskeletal ultrasonography (MUS) has proven to be helpful as it can show the thickening of the coracohumeral ligament and, in some cases, free fluid around the biceps tendon.
How Long Does A Frozen Shoulder Last?
A frozen shoulder can last anywhere from one to three years. The first stage – the freezing stage – can last anywhere between 2-9 months. The second stage – the frozen stage – can last from 4 months to a year.
The thawing stage can last anywhere from 5 months to 2 years. The symptoms of a frozen shoulder usually gradually subside over three years with minimal treatment.
Frozen Shoulder Pain Areas
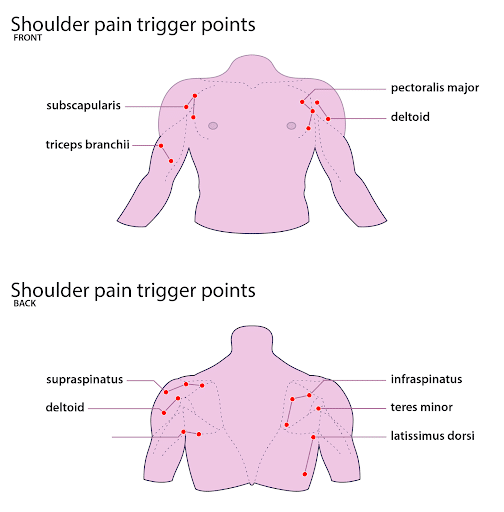
An individual can experience frozen shoulder pain along the muscle and fascia.The myofascial trigger points that arise due to a frozen shoulder are mostly in the rotator cuff muscles.
The rotator muscles are the subscapularis, supraspinatus, infraspinatus, and teres minor. In addition to these, there may be trigger points in the other shoulder muscles, such as the deltoids, biceps, and latissimus dorsi.
Massage therapy, dry fine needling, cupping, and the Graston technique are all therapies that target these trigger points and help relieve symptoms of a frozen shoulder.
Common Treatment Options For Frozen Shoulder
There are many treatment options for a frozen shoulder. Your doctor will recommend them based on your symptoms and symptom severity. The treatments are listed below:
Medications
Medications, such as acetaminophen and non-steroidal anti-inflammatory drugs (NSAIDs), are usually helpful in the initial freezing stage when there is inflammation. It’s important to note that these medications can provide short-term pain relief, however they may not be helpful for long-term pain relief.
Physical Therapy
Physical therapy is a treatment that provides long-term pain relief. Under the guidance of a trained physical therapist, exercise can help restore normal shoulder mobility.
Steroid Injections
Steroid injections are usually only considered for patients with moderate to severe pain. It may also be recommended to patients who are not responding to conservative treatments. A corticosteroid injection can be given directly into the shoulder joint capsule under ultrasound guidance (which helps correctly guide the needle).
Frozen Shoulder Manipulation
Manipulation under anesthesia (MUA) is a type of procedure that is usually only recommended when conservative treatments have failed. It can be performed in a hospital or ambulatory surgery setting.
During the procedure, the doctor manipulates the shoulder by moving the arm in order to break the adhesions and scar tissue that are restricting the joint. By manipulating the shoulder, the doctor can free up the frozen joint. MUAs are typically combined with an intra-articular steroid injection.
Recovery time after MUA depends on the severity of shoulder scarring, general health, and range of motion. MUAs are typically combined with an intra-articular steroid injection and physical therapy to help the success rates, which can last as long as 15 years for some people.
However, this procedure does come with risks. There is a risk of dislocation, fracture, blood clots, nerve damage, and injuries to the cartilage, labrum, and rotator cuff muscles during shoulder manipulation. Therefore, capsular distention is commonly preferred over shoulder manipulation under anesthesia (MUA).
Capsular Distention
Capsular distention, also known as hydroplasty, is a procedure in which the shoulder joint capsule is distended by filling it with fluid. At Centeno-Schultz Clinic (CSC), doctors use platelet-rich plasma (PRP) to distend the capsule.
The platelets in the plasma and the growth factors promote the repair and healing of the scar tissue in the joint capsule. It is usually done in the second stage of a frozen shoulder after symptoms have not improved despite a significant period of physical therapy.
Is this different from MUA? Absolutely! MUA is an aggressive shoulder manipulation procedure under a general anesthetic, which is then followed by a steroid injection. High dose steroids can damage both the cartilage and rotator cuff tendons especially after the six injections. At our Centeno-Schultz Clinic, high dose steroids are not used. Instead, our clinicians use PRP which is rich in growth factors and injected using ultrasound guidance.
Surgery
Arthroscopic surgery, also called an arthroscopic capsular release, is one of the last resorts for treating a frozen shoulder. In this procedure, the frozen joint capsule is divided so that there is more space for the joint to move. This procedure is done under general anesthesia.
How Physiotherapy Helps Frozen Shoulder Regain Movement
A physiotherapist can help you regain your shoulder mobility and flexibility. It can be used as adjunctive therapy along with medications and injections. The physiotherapist will start with gentle stretching exercises for the shoulder. They will work on stabilizing the joint and strengthening the muscles of the rotator cuff.
After strengthening exercises, patients can progress from isometric or static contractions, and then to exercises with a resistance band. Finally, they can move to free weights or weight machines. The physiotherapist may add posture exercises and other specific exercises for the deltoids and chest muscles.
Studies have shown that physical therapy can relieve symptoms of a frozen shoulder (2). At CSC, our physiotherapy team aims to restore the stability, articulation, symmetry, and neuromuscular function of the shoulder joint.
Functional Dry Needling
Functional dry needling, also known as intramuscular stimulation, is used to treat chronic pain in the shoulder. This treatment uses the same therapeutic needles as that of Chinese acupuncture, but the needles are only inserted in the shoulder muscles identified by the doctor (and not based on Chinese meridians). The needles are inserted into inflamed shoulder muscles to relieve trigger points.
Cupping Therapy
Cupping therapy is an ancient treatment where negative pressure is created using suction to stimulate the shoulder and upper back muscles. It done via cupping strokes. The strokes deeply penetrate the muscles and fascia to relieve pain.
There are two types of cupping: dry and wet cupping. In dry cupping, the skin is drawn into a suction cup. Dry cupping targets the muscle and deeper fascia, stretching out the deeper tissues. In wet cupping, lacerations are made in the skin to draw blood into the cup.
At CSC, only dry cupping is offered by our clinicians. Wet cupping is mainly aimed towards treating superficial pain.
Graston Technique
The Graston technique is a type of instrument-assisted soft tissue mobilization (IASTM). This technique is used to help increase range of motion in the joint, especially after a soft tissue injury.
A typical session lasts about 10 minutes. During each session, a trained practitioner will use dense stainless steel instruments to manipulate and stretch the shoulder muscles. This can help relieve any tension, tightness, and inflammation.
A person may need anywhere between 3-6 sessions to experience a noticeable reduction in shoulder symptoms.
Regain Shoulder Mobility By Treating Your Symptoms
Conservative therapy is the initial treatment of choice for a frozen shoulder. Surgery may be recommended when conservative options have failed. However, surgery carries significant risks, including the risk of bleeding, infection, failure, nerve injury, and rotator cuff injury.
At the Centeno-Schultz Clinic, our clinicians use regenerative therapies such as PRP to promote recovery from a frozen shoulder. The PRP injected into the shoulder distends the capsule and provides growth factors to facilitate healing. Regular physical therapy thereafter is important to maintain shoulder range of motion.
You don’t have to live with a frozen shoulder forever. It can be treated in a number of ways to help you regain shoulder mobility. At CSC, our board-certified doctors can recommend various treatments based on the symptoms of your frozen shoulder.
Do not disregard the symptoms you are feeling. Understand your condition with the help of our experienced team. Book yourself an appointment today!
John Schultz, MD
John R. Schultz M.D. is a national expert and specialist in Interventional Orthopedics and the clinical use of bone marrow concentrate and PRP for orthopedic injuries. He is board certified in Anesthesiology and Pain Medicine and underwent fellowship training. Dr. Schultz has extensive experience with same day as well as culture expanded bone marrow concentrate and sees patients at the CSC Broomfield, Colorado Clinic, as well the Regenexx Clinic in Grand Cayman. Dr. Schultz emphasis is on the evaluation and treatment of thoracic and cervical disc, facet, nerve, and ligament injuries including the non-surgical treatment of Craniocervical instability (CCI).
Other Resources for Frozen Shoulder
-
How To Release A Pinched Nerve In The Shoulder
A pinched nerve in the shoulder occurs when a nerve is compressed or irritated anywhere along its path, from the nerve root where it emerges from the cervical spine to the area in the shoulder it supplies. This can lead to shoulder pain, numbness, and pins and needles, and can even affect the movement of…
-
Treatment For A Torn Rotator Cuff Without Surgery: Exploring Your Options
Welcome to the Guide for Rotator Cuff Tear Relief Without Surgery. Rotator cuff injuries affect millions of people globally (1). The incidence vastly increases with age. Irrespective of the cause, there are many treatment options for rotator cuff injuries apart from surgery. If you want to avoid rotator cuff surgery, you’re in the right place!…
-
When Not to have Rotator Cuff Surgery? Know Your Options
It happened as you were playing racketball. There was loud pop followed by immediate pain. Moving your shoulder is almost impossible. What is the rotator cuff? What causes rotator cuff tears? What is rotator cuff surgery? When not to have rotator cuff surgery? Let’s dig in.What Is the Rotator Cuff? (4 Tendons) The rotator cuff…
-
KT Tape Shoulder: Facts You Need to Know!
KT Tape is used extensively for shoulder injuries. Dr. Schultz discusses what KT tape is, what it is used for, how it helps shoulder pain, whether it really works and a better solution.
-
Rotater Cuff Tear Surgery
Shoulder Pain Shoulder pain can come in many different forms and be caused by many different issues. Many structures exist in a small area making it more difficult to accurately diagnose what is causing pain without spending appropriate time to diagnose the issue. Common causes of shoulder pain include shoulder arthritis, acromioclavicular (AC) joint sprain…
-
MRI Images Showing Torn Rotator Cuff
What Is the Rotator Cuff? The Rotator Cuff is a group of 4 principal muscles that stabilize and support the shoulder joint. The four muscles, and their attached tendons that comprise the Rotator Cuff are the supraspinatus, infraspinatus, subscapularis, and teres minor, and any of these could be where we could find Rotator Cuff tears.…
-
Regenexx Rotator Cuff Tear Home Self-Exam
Hi It’s Dr. Centeno, and this is my series “You’ve Got the Power”, which is all about what you can do at home to understand why various issues are going on. In this episode, we’re going to cover why your shoulder hurts and focus on your Rotator Cuff. So, if you’re stuck at home, what…
-
Shoulder Pain from Lifting Weights
Lifting weights has many benefits. Shoulder pain from lifting weights can arise from many sources. Dr. Schultz discusses some of the unrecognized causes of shoulder pain and treatment options.
-
Rotator Cuff Surgery Recovery Timeline
If you’re considering surgery for a Rotator Cuff tear, an important thing to consider is how long, and what’s involved in, the Rotator Cuff Surgery Recovery Timeline. But let’s begin with the Rotator Cuff itself. What is the Rotator Cuff? The rotator cuff is a group of four muscles and tendons that stabilize the ball…
-
What to Expect from Shoulder Replacement Recovery
Many patients avoid shoulder replacement because they are concerned about shoulder replacement recovery. So what should you expect? How long does it take to recover from a shoulder replacement? Is shoulder replacement surgery successful? Let’s dig in. What is Shoulder Replacement Surgery? Shoulder replacement surgery, also known as shoulder arthroplasty, can be a transformative procedure…
References
- Struyf F, Mertens MG, Navarro-Ledesma S. Causes of Shoulder Dysfunction in Diabetic Patients: A Review of Literature. Int J Environ Res Public Health. 2022;19(10):6228. Published 2022 May 20. doi:10.3390/ijerph19106228
- X Chan HBY, Pua PY, How CH. Physical therapy in the management of frozen shoulder. Singapore Med J. 2017;58(12):685-689. doi:10.11622/smedj.2017107
- Akbar M, McLean M, Garcia-Melchor E, et al. Fibroblast activation and inflammation in frozen shoulder. PLoS One. 2019;14(4):e0215301. Published 2019 Apr 23. doi:10.1371/journal.pone.0215301
- Gianoukakis AG, Khadavi N, Smith TJ. Cytokines, Graves’ disease, and thyroid-associated ophthalmopathy. Thyroid. 2008;18(9):953-958. doi:10.1089/thy.2007.0405
- Bassett JH, Williams GR. Role of Thyroid Hormones in Skeletal Development and Bone Maintenance. Endocr Rev. 2016;37(2):135-187. doi:10.1210/er.2015-1106