Have you been suffering with neck pain but your imaging is normal? Two patients come to mind that I’ve seen recently whose cases can hopefully shed some light on this issue. These patients presented with very different symptoms, but were eventually found to have the same diagnosis! BUT importantly, both patients had “normal” imaging so their physicians told them that “nothing was wrong and their issues will resolve with time.” This is a problem because both of these patients actually had serious injuries and their physicians (and many insurance companies) dismissed their complaints and told them it was “just a sprain or strain and should resolve in a few weeks.” We see this too often and in these cases the true diagnosis is missed which leads to patients suffering unnecessarily before eventually getting to the right physician.
As physicians, we are taught that 70-90% of all patients’ problems can be discovered after discussing their history and doing a thorough examination (1-3). This is very true when it comes to orthopedic medicine. I find in practice that physicians do the exact opposite, if you have ever gone to an orthopedic office most of the time is spent getting x-rays and MRI’s before you even speak to a clinician, then the clinician (many times a PA or NP and not the MD/DO) reviews the imaging and tells the patient what is wrong with them without even discussing history or examining the patient!
Patient #1: 16 year old female high school athlete who was a back seat passenger during a car crash. The vehicle was hit from the side and the patient was thrown into the door on her right side and shortly after started having shoulder pain in the back of her shoulder with stiffness in her neck. She tried 6 weeks of physical therapy with no improvement. Her primary care physician told them nothing was wrong and that she should improve with time. She did not improve and an MRI of her shoulder and an X-ray of her neck were done and were read by the radiologist as “NORMAL” . Yet she couldn’t get back to her normal life which included competitive swimming and even things like sleeping and going to school continued to be difficult. I had previously treated her older brother, and her mother was tired of seeing her daughter in discomfort so she brought her in for an evaluation.
Patient #2: Middle age healthy (previously active) female who was involved in an altercation several YEARS ago that left her with debilitating pain at the base of her skull. Prior to the trauma was an avid runner and hiker but since the start of these issues she could barely walk a few blocks on flat ground before getting sharp pain in the base of her skull with debilitating headaches. The last several years she has been in and out of multiple doctor offices such as neurologists, orthopedic surgeons, neurosurgeons, non-surgical interventional spine physicians, and multiple physical therapists. She has been placed on multiple medications for headache, migraines and nerve pain but nothing has ever given her any relief. Nor did any physician ever give her a diagnosis, because all her imaging was read as “Negative.” Some physicians even suggested that this was “in her head.” She had to fly internationally from Europe to Broomfield, CO to finally get a diagnosis and a treatment plan aimed at getting her back to living a normal life again. She sent me this email while she was waiting to board her international flight to head home.
“I would also like to add, the last few days have been amazing and so inspiring for me and my recovery. I feel very privileged that I was given the opportunity to meet and be assessed by your team of clinicians, who truly focus on the patient’s functional recovery in such meticulous detail. With your help and all the additional insight you have given me, I am hoping I can push my recovery in the right direction again. As I mentioned during my visit, I’d felt completely abandoned by my local orthopedic consultants, who refused to give me a diagnosis and insisted I had no CCJ abnormalities. As a patient (and medical professional) I knew all along, I was really not right. But I was dismissed by every consultant I saw over the last 2+ years, to the point that I started to doubt myself, thinking ‘it might all be in my head’! What is so incredible, your team cleared up all my questions and concerns about my neck that I’d been searching for answers for nearly 3 years, literally within less than 24 hours of me arriving in Colorado! For that I cannot thank you and your team enough.”
Neck Pain but Your Imaging Is Normal?
So what is actually wrong with these 2 patients that all other healthcare providers couldn’t figure out?
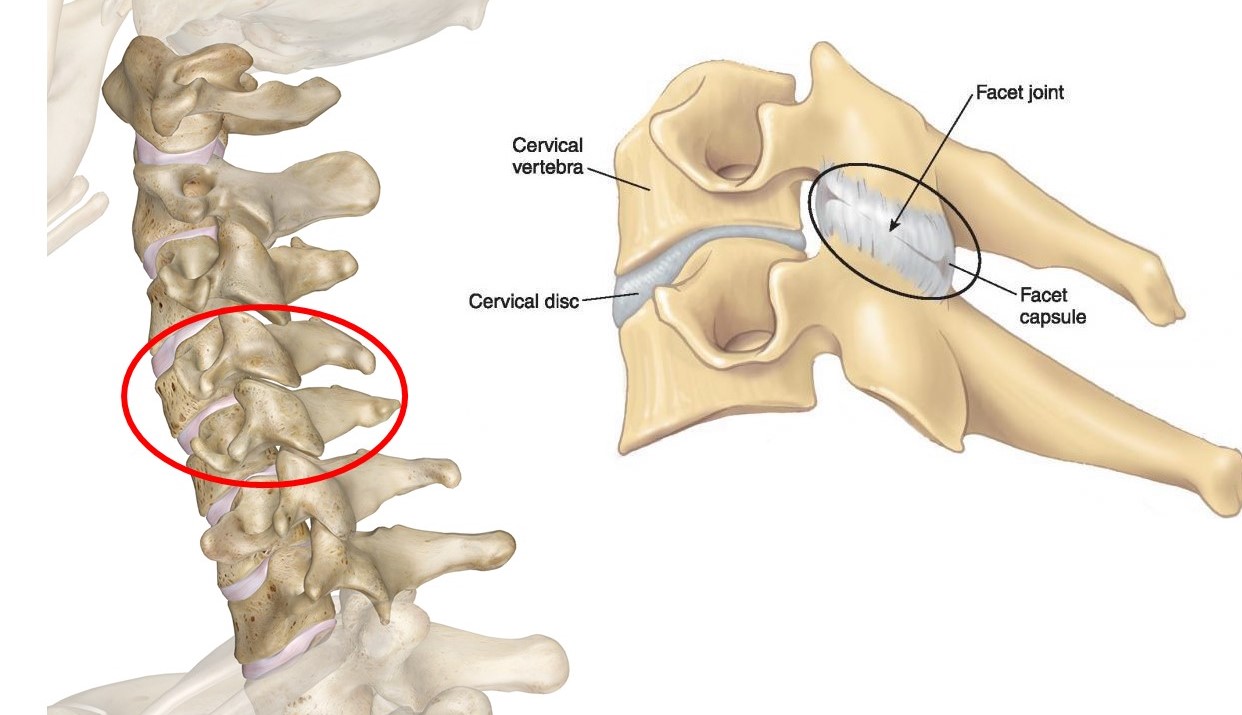
Facets are the joints that connect each vertebrae (back bones) together in your spine(1). Each vertebrae stack on top of each other and are connected by facet joints (one on each side). In the cervical spine you have 18 facet joints that connect your head to your spine, and each of the 7 cervical vertebrae that connect the cervical spine to the thoracic spine (mid back). These joints control the motion of your head and neck.
How are cervical facets damaged and what are cervical facet symptoms?
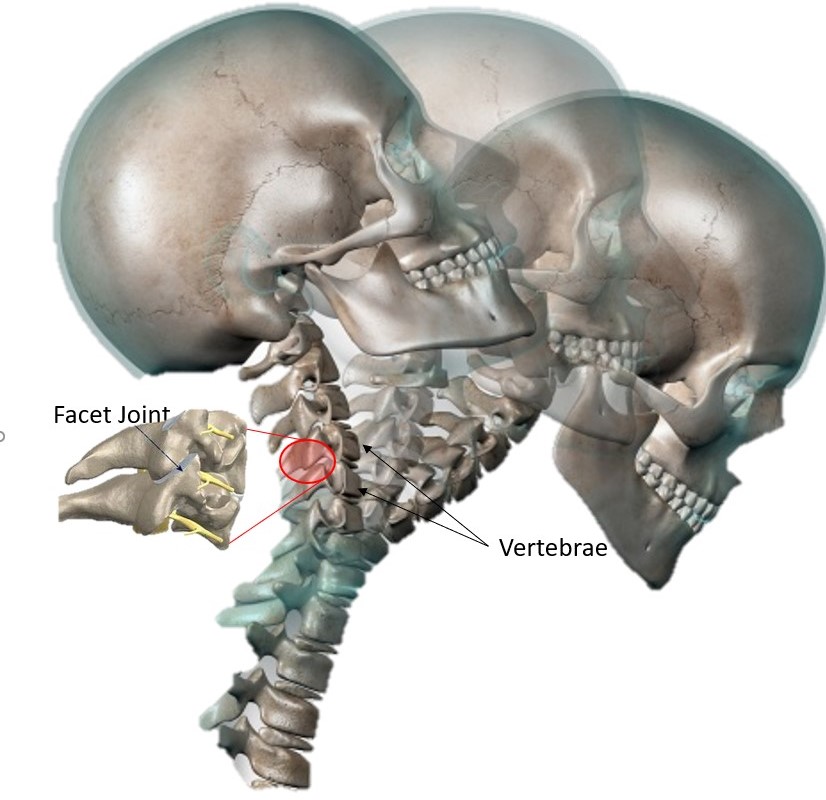
Whiplash is NOT a diagnosis but is the mechanism of injury! Both ladies had a form of whiplash injury. Understanding whiplash injuries is the key to understanding how and why they hurt. Any head trauma causes rapid forward and backwards motion of your neck (2,3). Whiplash injuries damage soft tissue such as the muscles, ligaments and tendons (4-6) but also causes compression of the facet joint leading to joint damage (7). Damage to these areas are not seen on simple x-rays and many times MRI’s are negative as well, but there is a host of literature detailing these injuries, which is why whiplash is a common finding in cases of head trauma that causes neck pain but your imaging is normal. Many physicians tend to believe that these injuries are “self-limiting” meaning they all resolve in a few weeks without any long-term consequences, but this idea is not supported by research (8-11). With 40-60% of individuals that suffer whiplash injuries report long-term (<6 month) pain and limitations compared to those that haven’t had whiplash injuries. Working with good physical therapist can help patients improve and prevent any long-term issues (12). But sometimes the damage to the facet joints and ligaments do not fully resolve and patients are left with chronic pain.
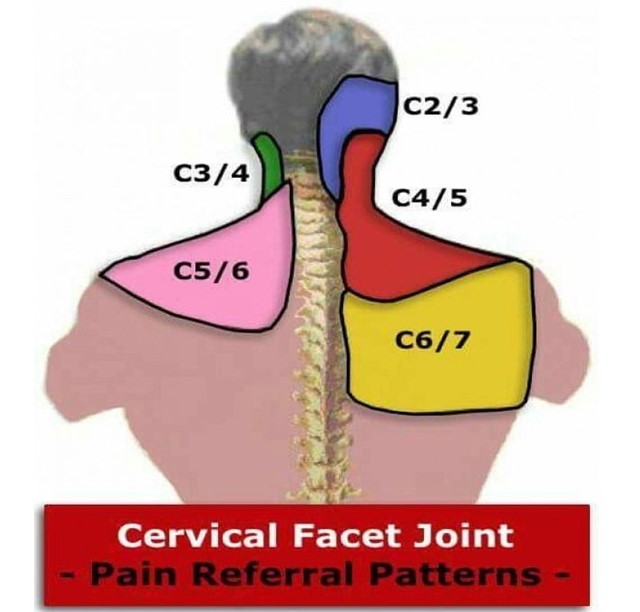
These injuries can cause pain in many different areas. See figure. This highlights where the pain from these joints can refer pain to. The facet joints can send pain signal to other areas outside the neck. This phenomenon is called “referred pain” (13) Classic example of referred pain is with heart attack patients. During a heart attack patient can describe left jaw pain and pain going down their left arm. There is nothing wrong with their jaw or arm but the nerves that innervate the heart also innervate those areas and the damage that is happening to the heart is interpreted by the brain as jaw and arm pain. The picture above shows where each facet joint can send pain signals to. As you can see, cervical facet pain can be manifest as headaches, neck pain, trapezium muscle pain, pain between the shoulder blades, pain in the shoulder and all areas in between!
Is there a treatment for cervical facet injuries?
Whiplash damages the following structures: facets, ligaments and other soft tissue structure. Physical therapy and other conservative treatment can be helpful (12). If conservative therapy fails can injections help? Commonly, corticosteroid injections are tried. The problem with steroids is that only offer short term relief (14) and can also be toxic to the tissue, leading to more damage to an already injured area (15).
When you have neck pain but you imaging is normal and you have finally gotten to a physician that has been able to accurately diagnose what’s going on, you need a treatment aimed at treating all the structures that are damaged! Through many years of experience, utilizing platelet-based therapies (PRP) and bone marrow concentrate (stem cells) are the best ways to treat whiplash injuries. Here is a video by Dr. Pitts outlining how these procedures in the cervical spine are completed. In patient 2 described above, I treated these upper facet joints given the fact that she had significant headaches associated with her neck pain. Dr. Schutlz has previously outlined how we go about treating the FSU – Functional Spine Unit. in treating lower back conditions, and we apply this concept to the cervical spine as well!
Follow Up On Patients Above:
Patient 1: We utilized her own growth factors (platelet rich plasma) isolated from her own blood, concentrated and used to treat her cervical facets, supporting ligaments and in addition we treated her shoulder rotator cuff and the deltoid muscles that attach to her shoulder. You can learn more about this treatment here. At 8 weeks post treatment, the patient was happy to result near 100% improvement / recovery and back in the pool swimming multiple times a week, prepping for her next competition, and back in school without any troubles! 😊
Patient 2: We treated with Regenexx SD along with platelet rich plasma into her cervical facets, ligaments and placed PL (platelet lysate) around certain nerves surrounding her neck that had become entrapped due to tight muscles and limited range of motion over the years…. She reported 80% improvement overall. Click here to learn more about her treatment:
“My occipital headache, which I constantly had to manage or put up with for over two and a half years since the day of my assault, was gone the day after the injections. My post-op neck stiffness resolved within around 10 days. I then noticed that I was able to regain my “top left quadrant” – looking up and left (head extension and left rotation).”
The Upside:
When you have neck pain but your imaging is normal and your neck pain hasn’t resolved, don’t give up! At CSC we set aside 1 hr for new patient evaluations, to sit down and listen to patients describe their history and then do a detailed examination to determine the extent of the injury. With whiplash injuries, while this is not a diagnosis, it is a mechanism of injury. These injuries can be very complex and contrary to many physicians, they are not self limiting nor do they resolve on their own. If left alone, they can have serious long-term implications (as in patient #2). We have excellent knowledge and skill on how to properly diagnose and treat these injuries using the most advanced regenerative medicine and injection techniques to aid in your recovery with the goal to get you back to living your life to the fullest!
If you have any questions about neck pain but your MRI is normal or feel like you are slow to recover from any other type of injury, feel free to contact us and we can assist in setting up time for an evaluation!
4. Kirpalani D, Mitra R. Cervical facet joint dysfunction: a review. Archives of physical medicine and rehabilitation 2008;89(4):770-4. 10.1016/j.apmr.2007.11.028 doi: 10.1016/j.apmr.2007.11.028.
5. Rydman E, Kasina P, Ponzer S, Järnbert-Pettersson H. Association between cervical degeneration and self-perceived nonrecovery after whiplash injury. The spine journal : official journal of the North American Spine Society 10.1016/j.spinee.2019.07.017doi: 10.1016/j.spinee.2019.07.017.
6. Chen HB, Yang KH, Wang ZG. Biomechanics of whiplash injury. Chinese journal of traumatology= Zhonghua chuang shang za zhi 2009;12(5):305-14.
7. Tominaga Y, Ndu AB, Coe MP, Valenson AJ, Ivancic PC, Ito S, Rubin W, Panjabi MM. Neck ligament strength is decreased following whiplash trauma. BMC musculoskeletal disorders 2006;7:103. 10.1186/1471-2474-7-103
8. Ivancic PC, Pearson AM, Panjabi MM, Ito S. Injury of the anterior longitudinal ligament during whiplash simulation. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society 2004;13(1):61-8. 10.1007/s00586-003-0590-3
10. Ita ME, Zhang S, Holsgrove TP, Kartha S, Winkelstein BA. The Physiological Basis of Cervical Facet-Mediated Persistent Pain: Basic Science and Clinical Challenges. The Journal of orthopaedic and sports physical therapy 2017;47(7):450-61. 10.2519/jospt.2017.7255doi: 10.2519/jospt.2017.7255.