Sacroiliac Joint Surgery is commonly done to treat SI joint instability and pain. Does it have any complications? Is it the best solution for the problem? In order to answer those questions, we need to start with the Sacroiliac Joint , or SI Joint, itself.
What Is the Sacroiliac Joint?
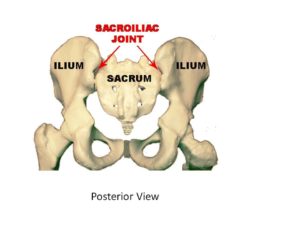
The sacroiliac joint is a very important joint formed by the sacrum and ilium bones and functions as a shock absorber between the spine and legs. It is a C shaped joint with the cartilage within the joint and an extensive number of supporting ligaments. Each patient has two sacroiliac (SI) joints. A left and a right. SI joint pain is common with an incidence of 15-30% of patients with low back (1). Patients that have undergone lumbar fusions are particularly susceptible to SI joint injury. A recent study reported that up to 75% of patients who undergo lumbar fusion will develop SI joint degeneration (2). Other causes of SI joint injury include trauma, degeneration, inflammation, pregnancy, ligament laxity and muscle weakness (3).
What Are the Symptoms of SI Joint Dysfunction?
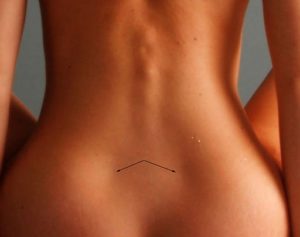
Pain is the most prominent symptom and typically involves the dimples of venus (4) It can also present as dull one-sided low back pain typically made worse upon standing from a seated position. If severe the pain can radiate into the buttock, posterior thigh extending down to the calf.
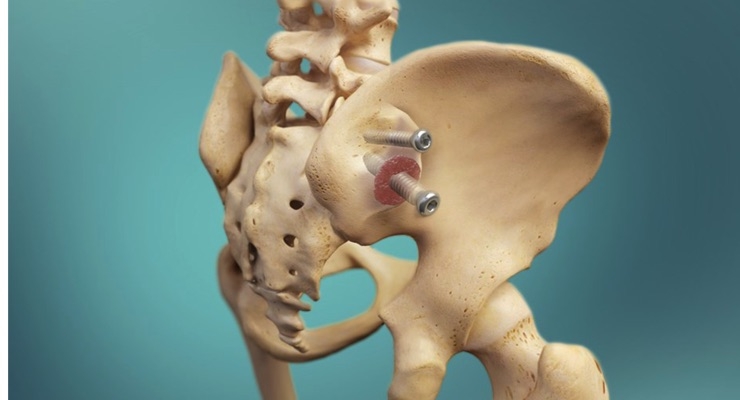
What Is Sacroiliac Joint Surgery?
SI joint surgery involves the fusion of the joint. Multiple implants are surgically inserted across the joint eliminating any movement. Remember that the joint is a critical shock absorber between the spine and legs and as such must be able to move.
How Successful Is Sacroiliac Joint Surgery?
A frequently quoted study demonstrated significant clinical benefit in those patients who underwent Sacroiliac joint surgery, which is a fusion, at 6 and 12 months (5). The results, however, need to be questioned as the study was a single-center and there no control groups after six months. Most alarming is that this study was sponsored by the company that manufactures the SI fusion hardware. In addition, some of the authors were paid. The lead author of the new two-year study was paid $72,007 by IFuse Implant, the maker of the SI fusion device (6). These issues are important and identify bias.
A recent study reported different outcomes (7). 469 patients who underwent SI joint fusion were followed from 2007 to 2014. The overall complication rate was 13.2 at 90 days which increased to 16.4% at 6 months. Patients also reported the onset of new low back pain after SI joint fusion with an incidence of 3.6% at 90 days and increased to 5.3% at 6 months.
A different 2015 study examined 16 peer-reviewed studies that involved 430 patients who underwent either open surgery or minimally invasive surgery for SI fusion (8). Re-operation rates after open surgery ranged from 0%-65% whereas in the minimally invasive surgery re-operation rate ranged from 0-17%. Major complications ranged from 5%-20% and in one study were found to be 56%.
Can We Learn a Lesson from Similar Types of Surgeries?
Yes! Lumbar fusion is a surgical procedure where two or more vertebrae are fused together with hardware. It is a common surgery for the treatment of low back pain and lumbar stenosis. There are many significant complications which have been reviewed in a previous blog. The most alarming is Adjacent Segment Disease where the discs and facets above and below the fusion are exposed to additional pressures resulting in wear and tear, degeneration. onset of pain and in some cases the need for additional surgery. Fusing a portion of the human body rarely makes sense and is commonly associated with new-onset of problems and pain typically 4-5 years after the original surgery. The same holds true for SI joint fusions. The fusion of this important shock absorber can result in new injuries in the lumbar spine, hip, opposite SI joint, and pubic symphysis. To learn more about Adjacent Segment Disease please click on the video below.
Non-Surgical Regenerative Treatment Options
Prolotherapy
Prolotherapy is the injection of natural irritants into joints, tendons, and ligaments to promote healing and improve stability. Concentrated dextrose is a common irritant used in prolotherapy. In a recent study patients with SI joint pain were randomized to undergo prolotherapy or steroid injections (9). At 2 weeks the pain and disability scores were similar whereas at 15 months the percentage of patients that reported pain relief of 50% or more was 58 % in the prolotherapy group and only 10% in the steroid group.
Platelet Rich Plasma & Stem Cells
Platelet-rich plasma is concentrated platelets and growth factors derived from whole blood. Blood is drawn from a peripheral site and placed into a centrifuge to remove red blood cells and concentrate platelets. PRP is an effective treatment option. PRP injections into the SI joint provided a marked improvement in joint stability, reduction in pain, and improved quality of life at 1 and 4 years post-treatment (10). Stem cell injections have also been effective in the management of SI joint pain (11). The Centeno-Schultz Clinic invented orthopedic stem cell injections and has extensive experience in the successful treatment of SI joint dysfunction with both stem cells and PRP.
The sacroiliac joint is an important joint that serves as a shock absorber between the spine and legs. It can be injured and become a source of significant pain and dysfunction. SI joint surgery involves fusing the joint, eliminating movement and the ability of the joint to function as a shock absorber. Studies that were not funded by the implant manufacturer demonstrated complications and the need for re-operation in some patients. Lumbar fusion is similar to SI joint fusion as it fuses as a critical shock absorber in the body. Lumbar fusion is associated with numerous complications that include Adjacent Segment Disease. Patients that undergo Si joint fusion have reported new-onset lumbar pain which most likely represents Adjacent Segment Disease. Prolotherapy, PRP, and stem cells can be effective treatment alternatives. Learn more about our treatment options for low back pain.
_________________________________________________
1.Grgić V. [The sacroiliac joint dysfunction: clinical manifestations, diagnostics and manual therapy]. Lijec Vjesn. 2005;127(1-2):30-5.
1.Sembrano JN, Polly DW. How often is low back pain not coming from the back. Spine. 2009;34(1):E27-32.DOI: 10.1097/BRS.0b013e31818b8882
2. Ha KY, Lee JS, Kim KW. Degeneration of sacroiliac joint after instrumented lumbar or lumbosacral fusion: a prospective cohort study over five-year follow-up. Spine. 2008;33(11):1192-8.DOI: 10.1097/BRS.0b013e318170fd35
3. Grgić V. [The sacroiliac joint dysfunction: clinical manifestations, diagnostics and manual therapy]. Lijec Vjesn. 2005;127(1-2):30-5.
4.Fortin JD, Falco FJ. The Fortin finger test: an indicator of sacroiliac pain. Am J Orthop. 1997;26(7):477-80.
5. Duhon BS, Cher DJ, Wine KD, Kovalsky DA, Lockstadt H. Triangular Titanium Implants for Minimally Invasive Sacroiliac Joint Fusion: A Prospective Study. Global Spine J. 2016;6(3):257-69.DOI: 10.1055/s-0035-1562912
6. https://projects.propublica.org/docdollars/
7. Schoell K, Buser Z, Jakoi A, et al. Postoperative complications in patients undergoing minimally invasive sacroiliac fusion. Spine J. 2016;16(11):1324-32.DOI: 10.1016/j.spinee.2016.06.016
8. Zaidi HA, Montoure AJ, Dickman CA. Surgical and clinical efficacy of sacroiliac joint fusion: a systematic review of the literature. J Neurosurg Spine. 2015;23(1):59-66.DOI: 10.3171/2014.10.SPINE14516
9. Kim WM, Lee HG, Jeong CW, Kim CM, Yoon MH. A randomized controlled trial of intra-articular prolotherapy versus steroid injection for sacroiliac joint pain. J Altern Complement Med. 2010;16(12):1285-90.DOI: 10.1089/acm.2010.0031
12.Sanapati J, Manchikanti L, Atluri S, et al. Do Regenerative Medicine Therapies Provide Long-Term Relief in Chronic Low Back Pain: A Systematic Review and Metaanalysis. Pain Physician. 2018;21(6):515-40.
Download Your free copy of Dr. Centeno’s groundbreaking work on spinal health and how Interventional Orthopedics can help you avoid life-altering surgery.