I’m an aging athlete with some SI joint instability. However, many patients have much more instability which can be disabling. So what is SI joint instability? How can it be treated? How does that intersect with my backcountry skiing? Let me explain.
What is SI Joint Instability?
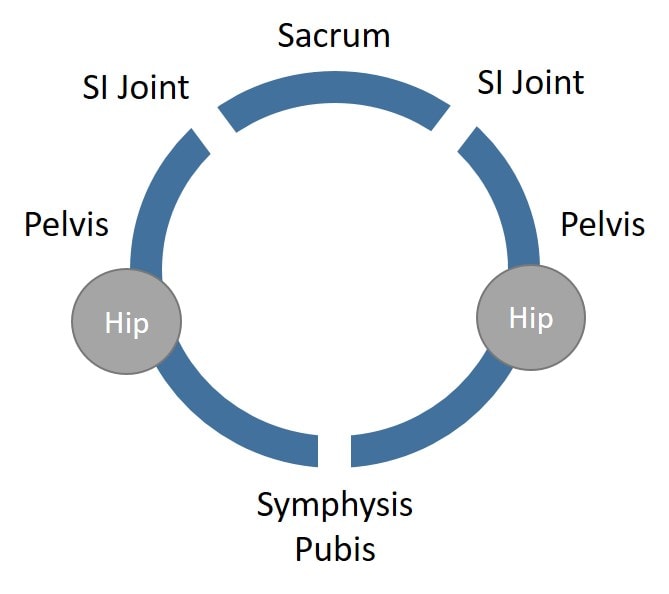
Your pelvis has three joints. You have two SI joints in the back and the symphysis pubis in the front. This is commonly called the “pelvic ring”. These joints are held together by tough ligaments. When these ligaments become stretched out due to wear and tear, congenital problems like hypermobility, or pregnancy and delivery, SI joint instability can ensue.
What’s instability? This means that the ligaments or muscles that stabilize the joints and keep them from moving too much aren’t doing their job. Hence the joint moves too much in the wrong directions and this can damage the joint surfaces.
Measuring SI Joint Instability is Tough
One of the reasons that patients are often misdiagnosed is that there is no readily available imaging test for SI joint instability. Meaning that no x-ray or MRI test can tell if your SI joints are unstable. There are research-based tests using ultrasound imaging, but this hasn’t made it to the clinic (1). Hence, the only way to tell if you have SI Joint instability is to have a doctor or highly trained manual therapist perform a physical exam, but even that presents a problem. Why? Only a tiny fraction of doctors or therapists are trained to be able to perform these tests and accurately diagnose the issue.
SI Joint Ligaments
The SI joint ligaments are the red-headed stepchild of the SI joint. Meaning many doctors will inject the joint itself with steroids (which can harm joint cartilage), but will never touch the ligaments. However, now that newer regenerative therapies are here that can tighten down the ligaments like prolotherapy, PRP, or stem cells, the SI ligaments are getting more attention (3,4).
Which Muscles are Involved?
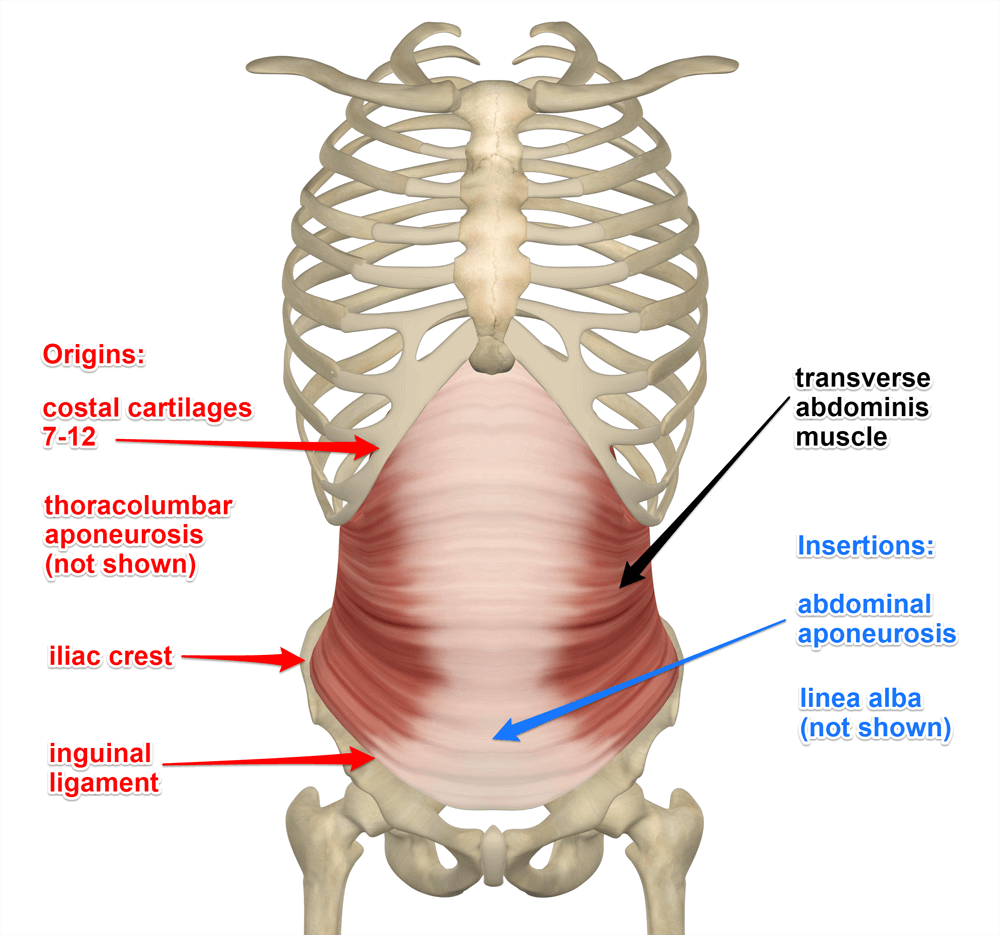
Studies have been done looking at which muscles reliably stabilize the SI joint. One of those is the transversus abdominus, which is a deep abdominal muscle (2). This is one of the muscles that contract when you perform “Kegel” exercises. This is also an important CORE muscle, so working on these types of exercises can also help stabilize the SI Joint. In the image here, all of the other abdominal muscles are stripped away. Note that the transversus is on the side of the abdomen in the flank area and deep to all of the other muscles. It runs horizontally unlike the obliques which run diagonally and live more superficially.
The Front of the Pelvic Ring is Critical for SI Joint Stability
Many patients with SI joint instability focus on the SI joints in the back of the pelvis. However, there’s even more going on in the front of the pelvis. Why? Remember that the pelvis is a three joint ring with the one in the front called the symphysis pubis. This joint can also be unstable in patients with SI joint instability, but it’s rarely even examined and even less often treated.
Why is the symphysis pubis so important? If we think about the pelvis as a ring with one joint in the front and two in the back, the two halves that come together in the front meet at the symphysis pubis (SP). Because of the simple physics of levers, if you can stabilize the symphysis pubis even a millimeter, that’s translated into more magnified movement in the SI joints. So treating the SP with injections that can cause the ligaments there to strengthen is often a critical step in treating SI joint instability.
How the Adductors and Lower Abs Impact the Syphysis Pubis and SI Instability
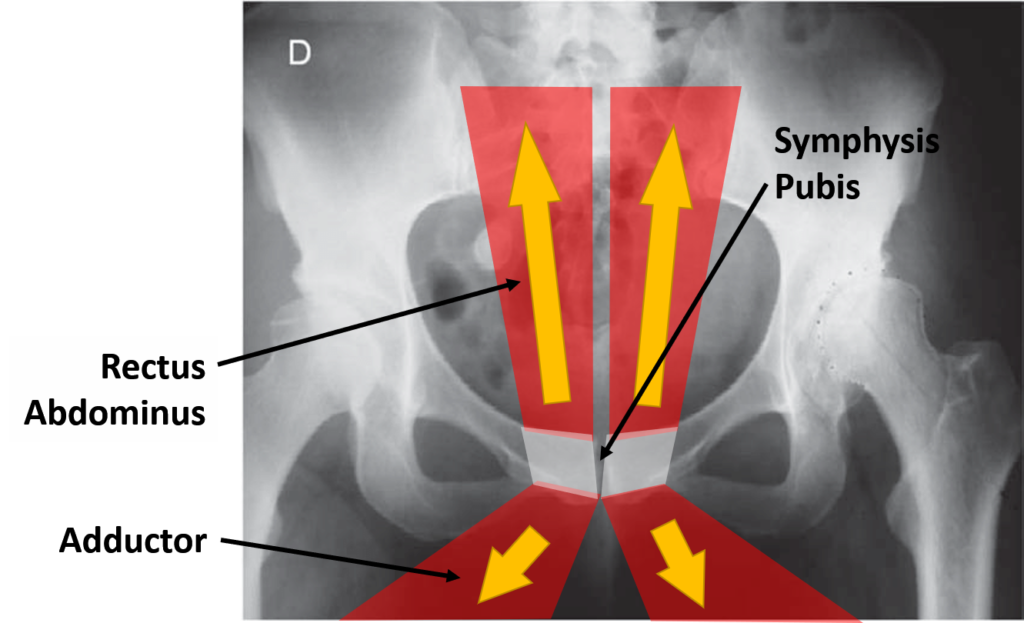
The muscles that attach directly to the symphysis pubis are the adductors and rectus abdominis. These muscles form one force couple, with the rectus abdominis pulling up and the adductor pulling down. They also share a piece of tendon that links the two muscles. Hence, it’s not hard to see how they would be involved in stabilizing the SP joint and therefore these are secondary stabilizers of the SI joints.
I recently had direct experience with these muscles. I love cross country skiing on backcountry trails behind our mountain home. Unlike nordic skiing on a golf course where there are nicely defined tracks, these trails tend to get a bit more beat up from snowshoe and hiking enthusiasts. Hence, without a groove to keep your skis going in one direction, you use allot of adductors to keep your leg from sliding outward.
One of my interesting observations is when I ski like this a few times, I tend to feel my lower abs all day while walking. This made sense as I thought about it, as there is no activating the adductors without also activating the lower abs (rectus abdominis). I also feel that my instability at the symphysis pubis gets better for a while (it’s only mild) after I ski.
What’s the take-home here? You can strengthen the pelvic ring by strengthening the muscles and this should work most of the time. Let’s review how that’s done.
SI Joint Stability Exercises
Lowest level:
- Kegel Exercises-These exercises work the pelvic floor muscles. For both men and women, they are the muscles that stop the stream of urination (more challenging for men). So you can dial them in and know you’re doing it right if you can accomplish that mid-stream. Alternatively, focus on those deep muscles that are at the base of your genitals to your anus. Hold and relax these muscles, which will also activate your transversus abdominis, a primary stabilizer of the SI joint. Start with 5 seconds on and off and then increase that to 30 seconds on and off ten times a day.
Next Low Level:
- Kegel exercises with Glute Bridges-Perform a Kegel exercise with a gluteal bridge as shown. Squeeze the gluts with the pelvic floor muscles at the top of the bridge. Use the repetitions and times as above.

Moderate Level:
- Adductor Squeezes-All of the above and add in a ball squeeze as shown. Focus on your adductors and lower abs. Do that 5 times to start and work up to three sets of 10. You can also add in a glute bridge as above (with the ball) while squeezing your glutes, pelvic floor muscles, adductors, and lower abs.

More Advanced:
- Gym-While Kegel exercises may help activate your transversus abdominis muscle and stabilize your SI joint from a muscular standpoint, treating SI instability should also involve your adductors and lower abs. A great way to do this at a gym is to work on the adductor machine while you focus on contracting your lower abs. If you’re doing this right you should feel tightness in the lower abs as you bring your legs together on the machine. You can also add a Kegal contraction with that same movement.
- Step outs with sliders-This is the toughest of all of these exercises, so it’s only for those who are more advanced. This is standing on one leg with the other leg on a slider disc. You contract your lower abs while you contract your glutes and pelvic floor while slowly sliding your leg out and back. You then do the other side. Start with 5 and work up to three sets of 10.

Injections to Stabilize the SI Joints and Symphysis Pubis
Exercises to stabilize the SI joint are always the first line of therapy. In addition, finding an expert manual physical therapist is a good bet as well. However, when all of that fails, the next step is injections to tighten down the ligaments in both SI joints and the SP. Again, treating all three joints in the pelvic ring is a good idea.
Ligament tightening can be accomplished using prolotherapy, platelet-rich plasma, or if all else fails, bone marrow concentrate (a same-day stem cell procedure). In fact, for some patients, until they get these joints tightened down, they may not be able to do any of these exercises. Hence, some patients may need to wait before starting exercise work.
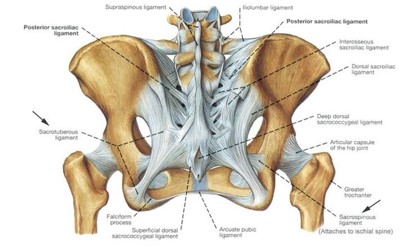
Shown here are the posterior SI ligaments in white. Note the extensive ligament complexes here that extend all the way from the lower spine to the bottom of the pelvis. These ligaments include the short and long dorsal SI joint ligaments, the sacrospinous ligaments, and the sacrotuberous ligaments. If you get these injected, the doctor should use a combination of fluoroscopy (real-time x-ray guidance) and ultrasound.
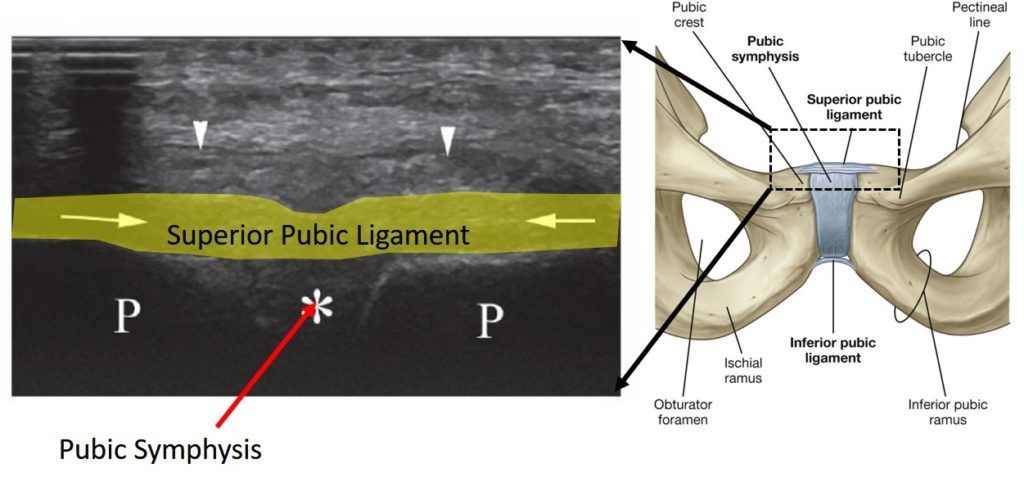
The symphysis pubis ligament injection can also be performed using ultrasound or with fluoroscopy. Below you see the superior public ligament that lives on the front of the symphysis pubis. On the left is what it looks like on the ultrasound image. This area is thoroughly numbed before the injection.
SI Joint Fusion

We have treated SI instability patients for decades and have only had a handful of patients who believed they needed an SI joint fusion after treatment for SI Joint Syndrome and SI Joint Instability. In this procedure, the surgeon places big screws through the SI joint so it doesn’t move. The problem? That motion needs to go somewhere, so this often wears out the hip or lower back at L5-S1, the two levels above and below. In addition, once you go down this road there is no going back, as the natural SI joint is destroyed by the procedure. Why? There are now three screws in it and if those are removed, that leaves three holes.
Make sure to read about the Perc-FSU procedure and our other alternatives to back surgery.
The upshot? SI joint instability can be fixed and treated. Hopefully, these concepts and these exercises are helpful. As an aging athlete, I need all the help I can get, so I think I’ll get back out on my skis again to engage the lower abs and adductors!
_______________________________________
References:
(1) Buyruk HM, Stam HJ, Snijders CJ, Laméris JS, Holland WP, Stijnen TH. Measurement of sacroiliac joint stiffness in peripartum pelvic pain patients with Doppler imaging of vibrations (DIV). Eur J Obstet Gynecol Reprod Biol. 1999 Apr;83(2):159-63.
(2) Richardson CA, Snijders CJ, Hides JA, Damen L, Pas MS, Storm J. The relation between the transversus abdominis muscles, sacroiliac joint mechanics, and low back pain. Spine (Phila Pa 1976). 2002 Feb 15;27(4):399-405.
(3) Singla V, Batra YK, Bharti N, Goni VG, Marwaha N. Steroid vs. Platelet-Rich Plasma in Ultrasound-Guided Sacroiliac Joint Injection for Chronic Low Back Pain. Pain Pract. 2017 Jul;17(6):782-791. doi: 10.1111/papr.12526. Si joint pain
(4) Kim W, Lee HG, Jeong CW, Kim CM, Yoon MH. A Randomized Controlled Trial of Intra-Articular Prolotherapy Versus Steroid Injection for Sacroiliac Joint Pain. The Journal of Alternative and Complementary Medicine 2010 16:12, 1285-1290.