Medicine is highly specialized now. Each specialty has a series of checkboxes that patient’s symptoms nicely fit into. For example, irregular heart rhythm with abnormal ECG is a cardiology problem. Shortness of breath with abnormal chest x-ray can be effectively evaluated and treated by a pulmonologist. Unfortunately, the symptoms and presentation of patients with upper cervical spine inatability do not fit nicely into any box. The irregular and often elevated heart rate is baffling to most cardiologists and most patients walk away with ” normal ” cardiac workup. So too with vertigo as the ENT specialist can find no explanation for their symptoms. Craniocervical Instability is real and can present with a number of symptoms that do not conveniently fit into a one specialists box. At the Centeno-Schultz Clinic we are committed to advancing a better understanding of this debilitating condition.
Where Is the Alar Ligament Located?
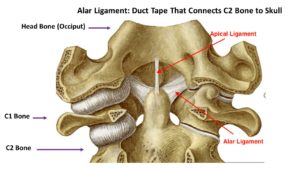
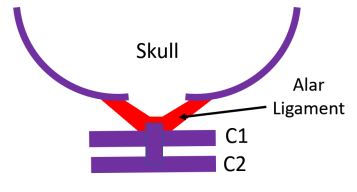
The Alar ligaments are paired ligaments located at the upper cervical spine. A ligament is a thick band of connective tissue. Think of them as duct tape. As such the Alar ligament is duct tape that holds your head onto your neck. More specifically it is the thick band of connective tissue that connects the skull to the C2 bone. Anatomically speaking the Alar ligament joins the occipital condyles to the Dens (C2 bone). They lie on either side of the Apical ligament. They are thickest at the Occipital attachment. Their orientation can oblique or horizontal (1)
What Is the Function of the Alar Ligament?
The function of the Alar Ligament is to stabilize the upper cervical spine, limit rotation and contra-lateral lateral flexion. Lateral flexion is side bending of the neck. An example would be stretching your neck to the side in an attempt to touch your ear to your shoulder.
How Many Alar Ligaments are There?
Each of us have two Alar ligaments. A right and left Alar ligament that work together to provide stability for the upper cervical spine.
Injury to the Alar Ligaments
Upper cervical spine injuries are common and mainly caused by car and sport accidents or falls (2). Rotation of the neck and/ or hyperflexion is common in Alar ligament injuries (3). Dvorak demonstrated that Alar ligament was extended the most while the head is rotated and bent forward (flexed) (4). It is most vulnerable to injury in this position. Examples include:
A rear-end car crash, especially one where the head hits the back window (e.g., a pickup truck)
A sudden jolt to the neck/head
Something falling on the head
Placing axial loads on the head (e.g., one patient who performed a neck exercise by arching his back to place his whole weight on the head)
The Alar ligament can be also be injured with an overly aggressive chiropractic adjustment.
Other causes of Alar ligament injury include cogential disorders with hypermobility of the joints and spine. A classic example is Ehlers-Danlos Syndrome (EDS).
What Is Craniocervical Instability (CCI)?
Injury to the Alar ligament can lead to upper cervical spine instability otherwise known as Craniocervical Instability (CCI). This is where there is excessive movement at the head neck junction. The upper neck facet joints (C0/C1, C1/2) become unstable and move around too much leading to injury and arthritis. This is turn recruits the muscles and tendons to work overtime to stablize the upper neck. Over time the muscles and tendons become overwhelmed and become injured and a source of pain and dysfunction.
Craniocervical Instability (CCI) is a medical condition characterized by injury and instability of the ligaments that hold your head onto the neck. The major ligaments involved are the Alar, Transverse and Accessory ligaments. It is a poorly understood condition that can be debilitating. Regretably it is often missed or misdiagnosed by medical providers. To learn more about CCI pleaseclick on the video below:
What Are the Symptoms of Alar Ligament Injury? (Feel Terrible)
Alar ligament injury can cause excessive movement between your head and neck. This in turn can cause movement and damage of upper cervical facet joints, discs, nerves, and blood vessels. Symptoms vary depending upon the severity of the ligament instability. In general the greater the instability the greater and more severe the symptoms. Common symptoms include.
1. Painful, Heavy Head
A constant to near-constant head pain that can be described as feeling like the head is too heavy for the neck to support. Many describe feeling like they have a “bobble-head”.
2. Headache
This is not your normal headache caused by your in-laws or excessive consumption of alcohol. This is a debilitating headache that is constant in duration and miserable. Headache is often caused by injury to the upper neck joints, muscles, and tendons due to ongoing instability.
3. Rapid Heart Rate
Elevated heart rate may occur as the Vagus nerve gets irritated by the extra motion in the upper neck. Another cause of elevated heart rate is Postural Orthostatic Tachycardia Syndrome (POTS). POTS is a medical condition that causes malfunction of the Autonomic nervous system. It is estimated to impact between 1,000,000 and 3,000,000 Americans. The Autonomic nervous system controls involuntary body functions such as heart rate and blood pressure. Malfunction of the Autonomic nervous system causes a number of symptoms which include rapid heart rate.
4. Brain Fog
Patients with CCI can struggle with memory, concentration, and ability to complete tasks. Every day can feel like your brain is stuffed full of cotton.
5. Neck Pain
Pain is typically localized at the base of the skull and aggravated bending forward and rotation. The pain can shoot up into the base of the skull, top of the head, forehead or behind the eyes.
6. Visual Problems
Visual disturbances can vary from mild to severe involving a number of different symptoms. Visual disturbances can happen because the upper neck supplies information to the brain to guide eye position and vice versa (5).
7. Dizziness
Balance problems can be a significant issue (6). Dizziness or imbalance is a feature related to the fact that the upper neck is a major contributor to balance (4). The upper neck provides position sense that has to be coordinated with balance information from the eyes and inner ear.
8. Chronic Fatigue
Excessive movement between the head and neck can cause irritation and dysfunction of the nervous system. The Autonomic nervous system is the most affected. A common symptom of autonomic dysfunction is chronic fatigue.
How Is an Alar Ligament Injury Diagnosed?
Regrettably, many clinics and providers focus on treating symptoms. Neck pain is not a diagnosis but rather is a symptom. At the Centeno-Schultz Clinic we are committed to understanding the underlying cause of your neck pain and dysfunction. An accurate diagnosis is critical. This will allow for a definitive treatment paln which in turn will allow for the best clinical outcomes. Diagnosing Craniocervical Instability (CCI) involves 7 main criteria which include:
Mechanism of Injury (How Did It Occur)
Understanding how and when the injury occurred is important. The two most common causes of CCI are trauma and medical conditions that cause people to have loose or compromised ligaments (8). Motor vehicle accidents, contact sports, and forceful manipulations by chiropractors are the most common examples of trauma. Ehlers Danlos Syndrome (EDS) is a group of inherited disorders that affect your ligaments and connective tissues (7).
Symptoms (Headache, Neck Pain and Neurologic Symptoms)
The symptoms associated with CCI can be extensive depending upon the severity of the instability. The most common symptoms include headache, upper neck pain, dizziness, visual disturbances, brain fog, fatigue, anxiety, visual challenges and elevated heart rate.
Physical Examination
In the age of managed care and 15-minute appointments, the art and practice of physical examination by a physician is almost gone. At the Centeno -Schultz Clinic all new patient evaluations undergo an extensive physical examination. Why? It is important to view the body as a whole and there are multiple potential physical findings in the neck, head, shoulder, and low back in patients with Cranial Cervical Instability.
Radiographic Studies for Cranial Instability ( Upper Neck MRI or DMX)
There are various types of radiographic studies which include x-ray, CT scan, and MRI. Unfortunately, traditional MRI and CT studies do not evaluate the upper cervical spine or alar and transverse ligaments. Special radiographic studies are required which include upper cervical MRI or rotatory CT scan. In addition, there are additional studies that involve the patient moving during the examination. These studies are useful to identify instability. Examples include upright MRI with upright flexion/extension. To see how this works please click on the video below.
Finally, a Digital Motion X-ray (DMX) is important in establishing the diagnosis of CCI. This is an x-ray examination that is recorded in which the patient is put through various movements including bending the neck forward, backward, and to the side. To learn more about DMX please click on the video below.
Response to Conservative Care
The common symptoms of CCI can also arise from different clinical conditions. For example, headaches with dizziness may arise from tight or contracted neck muscles. It is important that patients undergo conservative care such as rest, heat, stretching, physical therapy, massage, and chiropractic care. In some cases, symptoms improve with conservative therapy.
Response to Diagnostic Injections
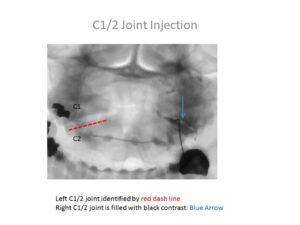
A diagnostic injection is a precise injection into a specific structure asking the question of whether or not it resolved the pain. Often times this is very helpful in the evaluation of patients with CCI. All diagnostic injections are performed under ultrasound or x-ray guidance, or both. Examples of diagnostic injections include:
Due to the severity of the symptoms, many patients are not able to complete their domestic or professional responsibilities. In severe cases of CCI, patients are confined to their homes and are socially isolated. The level of disability is important in evaluating and diagnosing Craniocervical Instability (CCI).
What Are the Treatment Options for Alar Ligament Injuries? (Conservative, Posterior Injections, Surgery)
There are three major types of treatment options. The specific type of treatment will depend upon the amount of instability and severity of symptoms.
Conservative
Patients with small amounts of instability can oftentimes be managed with conservative care. Conservative treatment options would include:
1. Upper cervical chiropractic care. Look for members of NUCCA (National Upper Cervical Chiropractic Association) 2. Physical Therapy 3. Bracing 4. Curve restoration. Look for chiropractors that specialize: Chiropractic BioPhysics.
Posterior Neck Injections
If conservative care fails to provide clinical improvement the next step is x-ray guided injections into the upper neck (8). Specifically, this would include injections into the Facet joints and Upper Cervical ligaments. An example would be the Supra and Interspinous ligaments that connect one vertebra to the next. Injections may utilize prolotherapy, PRP or Bone Marrow Concentrate. Not all injections are the same. There can be significant differences between clinics and practitioners. Accurate needle placement requires the use of x-ray and contrast. Contrast otherwise known as dye demonstrates where the needle it is. Equally important is it ensures that the needle is not in a blood vessel which can cause a serious complication. This is critical because if the needle is not in the targeted joint, the injected PRP or bone marrow concentrate will NOT magically get into the joint.
Surgery ( Fusion of Head to Neck)
If conservative care and injections fail many patients are referred for surgery.
There are many different types of surgical options all of which include Fusion. Fusion is a surgery that connects one or more segments of your spine together using screws, bolts, and plates. The goal is to provide stability. The most common is a Fusion of the head to the Cervical spine. This is illustrated in the picture to the right. It involves multiple screws and rods that are placed into the skull and neck. The procedure is major surgery with significant risks which include eventual arthritis above and below the Fusion, misplaced screws in nerves of Facet joints, and failure of the bones to fuse (non-union). Neck range of motion is permanently altered and, in most cases, severely restricted.
New Regenerative Treatment Option
In 2015 a nonsurgical treatment option for Cranial Cervical Instability was developed at the Centeno-Schultz Clinic. It involves the injection of a patient’s own bone marrow-derived stem cells into the damaged Alar, and Transverse ligaments. The procedure is very demanding and only performed at the Centeno-Schultz Clinic in Broomfield Colorado. The procedure is called Percutaneous Implantation of Cervical Ligaments (PICL) To learn more about this groundbreaking procedure please click on the video below.
In Summary
Medicine is highly compartmentalized with symptoms ideally fitting into checkboxes.
The symptoms and presentation of patients with Craniocervical Anstability do not fit the traditional checkboxes and therefore is often missed.
The Alar ligament is a paired ligament (a right and left) that is in the upper cervical spine.
The Alar ligaments function as duct tape to hold your head securely to your neck.
Injury of the Alar ligament can occur from trauma, overly aggressive chiropractic adjustments or due to congenital disorders.
Craniocervical Instability is medical condition characterized injury and instability of the ligaments that hold your head onto the neck. The major ligaments involved are the Alar, Transverse, and Accessory ligaments.
The symptoms of Craniocervical Instability are many and include headache, painful heavy head, brain fog, neck pain, vertigo, and fatigue.
There are 7 major criteria in diagnosing Craniocervical Instability.
Treatment options depend upon the severity of the instability and include when appropriate conservative care, injections, and surgery.
The PICL (Percutaneous Injection of Cervical Ligaments) is a breakthrough regenerative treatment option that allows appropriated identified patients to avoid surgery.
To learn more about the Alar ligament and Craniocervical Instability please download Dr. Centeno’s new book by clicking here.
If you or a loved one continue to suffer from headaches, dizziness, brain fog and chronic fatigue that has not responded to conservative therapy please schedule a telemedicine consultation. A board certified, fellowship trained physician will review your history, imaging and discuss appropriate treatment options.
6..Biesinger E. and Vertigo caused by disorders of the cervical vertebral column. Diagnosis and treatment. Adv Otorhinolaryngol. 1988; 39: 44– 51.
7.. Sobey G. Ehlers-Danlos syndrome – a commonly misunderstood group of conditions. Clin Med (Lond). 2014;14(4):432-436. doi:10.7861/clinmedicine.14-4-432
8.Centeno CJ1, Elliott J, Elkins WL, Freeman M. Fluoroscopically guided cervical prolotherapy for instability with blinded pre and post radiographic reading. Pain Physician. 2005 Jan;8(1):67-72. https://www.ncbi.nlm.nih.gov/pubmed/16850045