The upper neck and head pain was unrelenting and did not responed to conservative care or medications. Your doctor wants to refer you to a surgeon for possible fusion. What is the C1? What is the C2? What is the Atlantoaxial (AA) Joint? What are the key components of the AA Joint? What is a C1-C2 fusion? What are the indications for C1-C2 fusion? What is the Success rate of C1-C2 fusion? What are the complications? What are the regenerative treatment options? Let’s dig in.
What Is the C1? (Atlas)
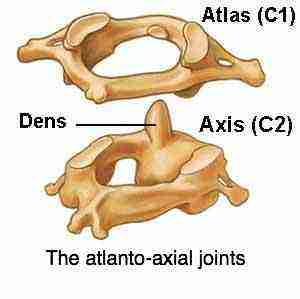
The C1 , also known as the Atlas is the first bone in your neck (1). It is named after the Greek God Atlas who held up the world on his shoulders. The Atlas plays an important role as your skull rests directly on this bone.
What Is the C2 (Axis)
Axis AKA C2 Bone
The C2 is the second bone in the neck and as such it is also referred to as Axis (2). It is an odd-looking bone as it has a boney peg that looks like the Washington Monument. This boney projection is called the Dens. The Dens extends upward to the Atlas bone. It provides a stable point upon which the Atlas bone can rotate.
What Is the Atlantoaxial (AA) Joint?
The AA joint is formed by the union of the C1 and C2 bones. The Atlantoaxial joint is composed of three smaller joints:
Medial AA joint
This is a pivot type joint and is formed between the Dens and ring of the C1 bone.
Two Lateral AA joints
Bilateral joints formed by the C1 and C2 bones. A joint is formed when two bones come together. Think of where the thigh bone meets the shin bone. The two bones come together to form the knee joint. So too with the C1 and C2 bones. They come together and form a joint. Like the knee joint, the AA joint is lined with cartilage.
What Are the Key Components of the AA Joint?
Cartilage
The AA Joint is lined with cartilage. Cartilage is the white shiny surface on the end of a bone that enables the smooth, pain-free movement of the joint. It absorbs and distributes large compressive and shear forces. The AA Joint is susceptible to injury and degeneration resulting in pain and reduced range of motion.
Ligaments
Ligaments are thick pieces of connective tissue that connect bone to bone. They provide support and stability. The key ligaments include the Alar, Transverse and Apical ligament.
Capsule
The AA Joint has a capsule that covers the entire joint, It is a saran wrap-like covering composed of fibrous connective tissue. It provides support, distributes the forces, and limits the range of motion.
Muscles
The are a large number of small muscles in the upper neck. They provide important support, stability and enable motion such as bending forward, backwards and rotating. One of the muscles called the Rectus Capitus Posterior Minor (RCPM) plays a very important role. It actually connects to the covering of the brain (3). It is called the Myodural Bridge. Clinically physicians have found that a tight or dysfucntional Rectus Capitus Posterior Minor muscle can put pressure on the Dura resulting in severe headaches.
What Is C1-C2 Fusion? (A Major Surgery)
A Fusion is major surgical procedure where a two or more spinal bones are permanently connected to one another. The goal is provide stability in an unstable situation. Rods, screws and plates and bone grafts are used during fusion surgery. A C1-C2 Fusion involves permanently uniting the C1 and C2 bones together using hardware. There are different surgical approaches which include from the front of the spine ( anterior) and from the back ( posterior).
What Are the Indications for C1-C2 Fusion? (Fracture, Tumor, AA Joint instability)
There are many indications for C1-C2 Fusion. The most common include:
C2 Complex Fractures (5)
Like all bones, the C1 and C2 bones can be fractured. There are different types and severity of fractures which can jeopardize AA joint stability and function.
Tumors Involving C1 or C2
Tumors can arise from within the C1 or C2 bone or adjacent to them. The tumors can compromise the spinal cord, neural function and AA joint stability.
Advanced Inflammatory Conditions
Rheumatoid Arthritis is an autoimmune disease that can compromise the C1-C2 joint. It is a conditon where the body’s immune system attackes its own tissue including joints.
Atlantoaxial Joint Instability is a medical condition where there is excessive movement at the junction of the C1 and C2 bones. This instability can cause a significant number of symptoms and can damage the spinal nerves and spinal cord. Atlantoaxial Joint Jnstability can arise due to trauma or cogenital instability such as patients with Ehler Danlos Syndrome or some variation of hypermobility.
Atlantoaxial Joint Instability (AAI)
Step 1
Imaging-Get movement based imaging
(DMX or Upright MRI with flexion and extension).
Step 2
Get Typed via a Telemed Appointment-There are 8 different types of CCI based on which
ligaments are Injured.
Step 3
Exam-If you’re a candidate for precise orthobiologic injections, you fly in for an exam and
treatment. A hands-on exam refines what we need to treat.
Step 4
Treatment-Get treated with a CCI focused, orthobiologic treatment plan tailored to you. That
includes PICL or whichever image guided, precise injections are the most likely to help you.
Determining the success rate of C1-C2 Fusion is a difficult as there are several different indications for C1-C2 Fusion. These can impact the ” success” of the surgery. Furthermore there are different surgical approaches to fusing the C1-C2 bones. Examples include using an anterior approach vs the posterior approach. The type and composition of the implanted hardware (screws and plates) can also vary. The surgery is technically demanding due to the tight space and number of important nerves and blood vessels in close proximity to the C1-C2 joint. A brief review of the literature reveals:
Using a poliaxial screw in the C1 latereal mass and C2 pedicle Bourdillon demonstrated 85% of the screws were correctly positioned and resulted in a 100% fusion rate in a study group of 26 patients (4).
Other studies have demonstrated fusion rates as low as 35-40% (5a).
Fusion is a commonly used metric of success in most surgical literature. There are many other important factors that are not evaluated or extensively discussed in the surgical literature which include:
Pain
Reduced Range of Motion
Headaches
Numbness
Ability to perform activities of daily living
While a given surgery may be result in “successful fusion” there can be significant complications which are discussed below. These can signficantly impact patient well being.
C1-C2 Fusion Complications
C1-C2 Fusion is a technically demanding surgery. Like all surgeries there can be complications. The most common include:
Misplaced Screws
Surgical screws are placed into the C1 and C2 bones to stabilize the joint. These bones espically the C1 bone are small in size. Fractures complicate matters. The screws can be placed incorrectly resulting in tissue damage, nerve and blood vessel injury (5).
Screw loosening
The surgical screws can loosen over time damaging adjacent tissue and compromsing the stability of the AA Joint. Treatment often times requires additional surgery.
Failed Fusion (Non-union)
Fusion involves permanently uniting the C1 and C2 bones. The inserted surgical hardware stabilizes the AA Joint promoting bone growth between the C1 and C2 bones. Unfortunately the bones do not always fuse together. This is referred to as a non union and most often requires additional surgery. OUCH!
Adjacement Segement Disease (ASD)
Adjacent Segment Disease is a common condition that occurs after fusion surgery. Our discs and facet joints absorb the forces of dailing living. Fusion eliminates one or more of these shock absorbers. This in turn causes additional pressure to the discs and facets above and below the fusion. These additional forces can result in injury and breakdown of the adjacent discs and facet. The end result often times is pain and restricted movement. Treatment options include extending the fusion an additional level. To learn more about Adjacent Segment Disease please click on the video below.
Nerve Injury
Nerves provide important information to our bodies. They are very fragile and susceptible to injury by compression, traction or being accidently cut. The Occipitial nerve can be compressed by faulty placement of the surgical screws resutling in debilitating Occipital headaches (6). In some surgical approaches the C2 nerve is intentionally cut which is associated with a high risk of postoperative numbness.(7)
Vascular Injury
Arteries and veins provide critical blood supply and drainage to the brain and neck. Both are susceptible to injury during C1/2 fusion. Vertebral Artery injury is a documented complication from C1/2 fusion.
A known complication is Vertebral Artery injury (8). The Vertebral Artery provides important blood supply to the neck and brain.
Regenerative Treatment Options
The Physicians of the Centeno-Schultz Clinic are experts in the treatment of Atlantoaxial Instability and other upper neck injuries that are due to mild to moderate instability and joint injury. Treatment starts with establishing a correct diagnosis. This involves reviewing past medical history, traumatic history, onset and duration of current symptoms, treatment to date and appropriate radiograhic studies. Treatment options include x-ray guided injections of PRP or bone marrow concentrate into the Atlantoaxial (AA) Joint and support ligaments. In some cases bone marrow concentrate is injected directly into the Alar and Transverse ligament. The procedure is called a PICL which stands for Percutaneous Implantation of CranioCervical Junction Ligaments. This is a complex procedure that is only performed at the Centeno-Schultz Clinic in Broomfield Colorado. To learn more about this procedure please click on the video below.
In Conclusion
The upper neck is composed of a series of boney building blocks that are numbered.
The C1 also known as the Atlas is the first bone in the neck.
The C2 is the second bone in the neck and is also referred to as the Axis.
The Atlantoaxial (AA) Joint is the union of the C1 and C2 bones.
The AA Joint is composed of cartilage, ligaments, capsule and muscle.
A C1-C2 fusion is a major surgery uniting the C1-C2 bones together with implanted hardware such as screws and plates.
The major indications for a C1-C2 Fusion are fracture, tumor and Atlantoaxial Joint Instability.
Success is difficult to access due to the different indications and surgical approaches.
Successful is a commonly used metric in the surgical literature but does not address pain, range of motion or patient satisfaction.
We can’t discuss the success rate of C1-C2 Fusion without discussing C1-C2 Fusion complications. They include misplaced screws, screw loosening, failed fusion, Adjacent Segment Disease, nerve injury and vascular injury.
The Centeno-Schultz Clinic are experts in the treatment of Atlantoaxial Joint and other upper cervical joint injuries without surgery. Treatment options include PRP and bone marrow concentrate.
3.Zheng N, Chung BS, Li YL, Liu TY, Zhang LX, Ge YY, Wang NX, Zhang ZH, Cai L, Chi YY, Zhang JF, Samuel OC, Yu SB, Sui HJ. The myodural bridge complex defined as a new functional structure. Surg Radiol Anat. 2020 Feb;42(2):143-153. doi: 10.1007/s00276-019-02340-6. Epub 2019 Sep 28. PMID: 31563971.
4.Bourdillon P, Perrin G, Lucas F, Debarge R, Barrey C. C1-C2 stabilization by Harms arthrodesis: indications, technique, complications and outcomes in a prospective 26-case series. Orthop Traumatol Surg Res. 2014 Apr;100(2):221-7. doi: 10.1016/j.otsr.2013.09.019. PMID: 24629457.
5.De Iure F, Donthineni R, Boriani S. Outcomes of C1 and C2 posterior screw fixation for upper cervical spine fusion. Eur Spine J. 2009;18 Suppl 1(Suppl 1):2-6. doi:10.1007/s00586-009-0981-1
6.Stillerman CB, Wilson JA. Atlanto-axial stabilization with posterior transarticular screw fixation: technical description and report of 22 cases. Neurosurgery. 1993 Jun;32(6):948-54; discussion 954-5. doi: 10.1227/00006123-199306000-00011. PMID: 8327097
7. Huang DG, Hao DJ, Li GL, Guo H, Zhang YC, He BR. C2 nerve dysfunction associated with C1 lateral mass screw fixation. Orthop Surg. 2014;6(4):269-273. doi:10.1111/os.12136