Anterior Cruciate Ligament Injuries and Treatments
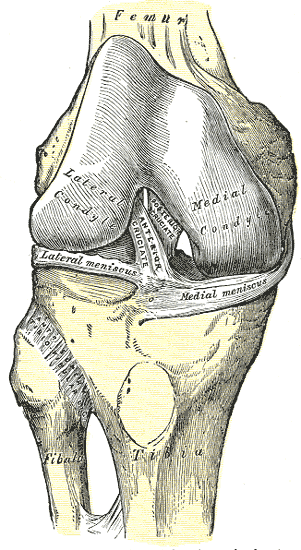
The ACL (anterior cruciate ligament) is an important knee stabilizing ligament. It prevents the tibia from moving too much frontward (anterior translation) and twisting too much (internal rotation). It is under most stress with landing from a jump, or a planted foot with twisting, and this is how it can be injured. It can commonly be injured with a cut in soccer or basketball or direct blow to the knee. Tears of the ACL can be classified as partial, complete but non-retracted, complete and retracted. Some small partial tears could be treated with just physical therapy and strengthening to compensate. Sometimes despite a larger tear, some people can just do physical therapy and be able to “cope” with an ACL tear. However, traditionally most ACL tears are treated via surgery (ACL reconstruction) especially in athletes.
ACL Reconstruction Surgery and Limitations
With surgery, the old ACL is taken out and replaced with an autologous tendon graft. This means a tendon in the same patient such as the patella, quad, hamstring, or IT band. Sometimes a cadaver tendon is used. It usually takes 9 months to 2 years to fully recover and potentially get back to sports for athletes. Even still many will not return to the same level of sport, or, if they do their careers are shortened. Return to sports occurs in 81% of patients, 65% to preinjury level, 55% return to competitive sports1. One study showed there was no difference in return to sports versus just physical therapy2.
Want to Get Back to What You Love, Without Surgery and Medication?
ACL Injuries in Teens and the Chance for Osteoarthritis by Age 30
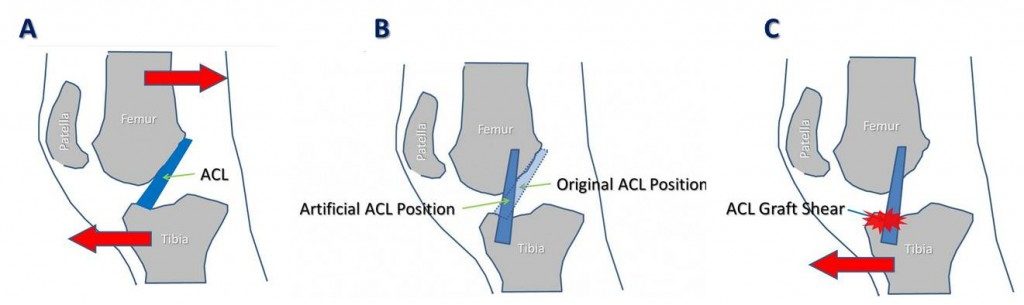
In young patients 2/3rds will end up with Osteoarthritis by age 303! For any age, 20-50% of patients with have arthritis in 10-20 years. Many patients and parents do not realize that after ACL surgery that knee is never quite the same. A normal ACL has 2 bundles that give it strength and nerve fibers to help tell your brain where the knee is in space. It also is at a certain angle to prevent both excess anterior (front) and rotational movement of the tibia (lower leg bone). A post-surgical ACL graft will only have one bundle placed at a steeper angle mostly helping with front motion only, it will have lost important nerve fibers to help with proprioception, and multiple studies show strength deficits after surgery. Additionally, if a graft was taken from the same knee, that site with be weaker.
ACL Surgery Alternatives
Because of these limitations of the surgery, we created our Perc-ACLR procedure to assist the body heal ACL tears. This involves injecting bone marrow concentrate containing stem cells precisely into the ACL with X ray guidance to stimulate repair of the ACL. This preserves both bundles of the ACLs, keeps the nerve fibers, and maintains the appropriate angle of the ACL. We have published peer-reviewed research on the success of this technique4,5, shown many successful before and after images and are completing a randomized controlled trial showing the effectiveness as well. This procedure can promote the body to heal ACL tears that are partial or complete non-retracted tears which are about 70% of ACL tears. However, complete retracted tears still need surgery. Early success rates have been about 83% with a re-tear rate of 4%4.
Second ACL Tear of the Same Knee
Because of the limitations listed above for ACL surgery, there is a risk of re-tearing the ACL after surgery. Retear rates can vary widely from 9% to 30%6.
One study showed 29% of patients with ACL surgery had a second tear within 2 years. The rate of ACL tears in patients who had the surgery compared to healthy patient controls was 5-6 times higher. Furthermore, in women there was a 2x more likelihood of tearing the opposite ACL after having one surgical reconstruction7.
In another study Patients that had surgery had a 15 times higher risk of another ACL surgery compared to controls. Females again were more likely to retear the same ACL and the contralateral one.
Another study showed that allografts (cadaver grafts) had higher rates of retear compared to autograft (using a tendon from the same patient)8.
Other factors for second ACL tear
One of the reasons for a second tear of the ACL is because of poor biomechanics. This means abnormal hip or knee angles, asymmetric weakness in muscle groups, or landing in an awkward position at the knees. Women have a higher risk for some of these factors since they tend to have wider hips than men and that increases the angle form the hip to the knee. When women or men with weaker outside hip muscles land, the knee tends to rotate inward putting more stress on the ACL. To correct these things any one after an ACL injury should be doing extensive physical therapy to not only strengthen but to work on symmetry, landing technique and reducing the stress on the knees. Really, any athlete or someone involved in “cutting” sports should consider working with a trainer or physical therapist to see if they have any of these biomechanical problems and fix them to reduce chances of the first injury!
How to treat a second ACL tear
Treatment of a retear of the ACL is similar to treatment the first injury. Partial tears of the ACL graft can be treated with our Perc-ACLR procedure. Complete retracted tears would require another surgery. If a second surgery is needed then it will likely be a bigger deal since the bones have already been drilled into. Also, often a cadaver graft is used which is less strong compared to allograft (a graft from the patient’s own body). Sometimes, if a patient is able to do enough physical therapy to strengthen the knee and work on biomechanics, they can learn to live with the ACL completely torn, they just most likely would need to avoid “cutting” sports. Our Perc-ACLR procedure can be used in conjunction with surgery (Regenexx ACL Repair vs Reconstruction Surgery for Knee ACL) as well to try to improve healing and reduce the rate of re-tear.
Bottom Line
The ACL is an important stabilizing knee ligament. It can be injured with “cutting” sports or direct trauma. Risk factors are being a women or having poor biomechanics. Traditionally surgery was the only treatment option besides physical therapy. Now with our Perc-ACLR procedure we can treat about 2/3rds of the typical surgical candidates as long as the tear is not complete with retraction. The Perc ACLR procedure can also be done after surgery to enhance outcomes. If you do tear your ACL and have surgery or the Perc ACLR procedure there is a chance of re-tear. Those tears can again be treated with the Perc ACL procedure or with another surgery if a larger tear. Some ACL tears and re-tears can be treated just with physical therapy to compensate in a few patients we call copers. If you or anyone you know has an ACL tear or re-tear they can contact the Centeno Schultz clinic to see what their treatment options are.
References
- Grindem H, Eitzen I, Engebretsen L, Snyder-Mackler L, Risberg MA. Nonsurgical or Surgical Treatment of ACL Injuries: Knee Function, Sports Participation, and Knee Reinjury: The Delaware-Oslo ACL Cohort Study. J Bone Joint Surg Am. 2014 Aug 6;96(15):1233-1241. doi: 10.2106/JBJS.M.01054. PMID: 25100769; PMCID: PMC4116562.
- Sepúlveda F, Sánchez L, Amy E, Micheo W. Anterior Cruciate Ligament Injury: Return to Play, Function and Long-Term Considerations. Curr Sports Med Rep. 2017 May/Jun;16(3):172-178. doi: 10.1249/JSR.0000000000000356. PMID: 28498226.
- Dare, D., Rodeo, S. Mechanisms of Post-traumatic Osteoarthritis After ACL Injury. Curr Rheumatol Rep 16, 448 (2014). https://doi.org/10.1007/s11926-014-0448-1
- Centeno C, Markle J, Dodson E, Stemper I, Williams C, Hyzy M, Ichim T, Freeman M. Symptomatic anterior cruciate ligament tears treated with percutaneous injection of autologous bone marrow concentrate and platelet products: a non-controlled registry study. J Transl Med. 2018 Sep 3;16(1):246. doi: 10.1186/s12967-018-1623-3. PMID: 30176875; PMCID: PMC6122476.
- Centeno CJ, Pitts J, Al-Sayegh H, Freeman MD. Anterior cruciate ligament tears treated with percutaneous injection of autologous bone marrow nucleated cells: a case series. J Pain Res. 2015;8:437-447. Published 2015 Jul 31. doi:10.2147/JPR.S86244
- Sanders TL, Pareek A, Hewett TE, Levy BA, Dahm DL, Stuart MJ, Krych AJ. Long-term rate of graft failure after ACL reconstruction: a geographic population cohort analysis. Knee Surg Sports Traumatol Arthrosc. 2017 Jan;25(1):222-228. doi: 10.1007/s00167-016-4275-y. Epub 2016 Aug 13. PMID: 27522592.
- Paterno MV, Rauh MJ, Schmitt LC, Ford KR, Hewett TE. Incidence of Second ACL Injuries 2 Years After Primary ACL Reconstruction and Return to Sport. Am J Sports Med. 2014 Jul;42(7):1567-73. doi: 10.1177/0363546514530088. Epub 2014 Apr 21. PMID: 24753238; PMCID: PMC4205204.
- Widner M, Dunleavy M, Lynch S. Outcomes Following ACL Reconstruction Based on Graft Type: Are all Grafts Equivalent? Curr Rev Musculoskelet Med. 2019 Dec;12(4):460-465. doi: 10.1007/s12178-019-09588-w. PMID: 31734844; PMCID: PMC6942094.