Even a small meniscus tear can make walking difficult for you. If you are experiencing any of these symptoms, you may want to seek medical help as soon as possible, depending on the type of tear you have. Needless to say, a lot depends on understanding the meniscus tear types there are and what each might mean for treatment options.
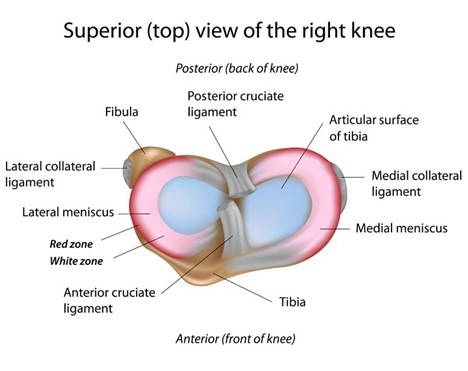
The meniscus is a fibrocartilage structure that sits on top of the tibia (lower leg bone). There is one on the medial (inside) aspect of the knee, one on the lateral (outside) aspect of the knee. It is shaped like a C and provides some cushion and support for the knee joint as it acts as a shock absorber.
A meniscus can be torn with a particular injury typically with sports, twisting, deep knee bending, rotating, or high-intensity type activities. Also, it can just gradually tear or wear out through degeneration throughout the years as we age.
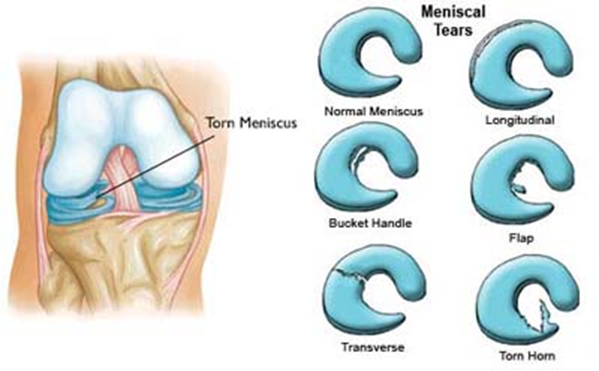
Those degenerative tears can be found on most MRIs but are generally not of clinical relevance (1). There are 6 main types of meniscal tears: horizontal (longitudinal), radial (transverse), intrasubstance, bucket-handle, flap tear, and complex tear. For more information on the meniscus and knee problems read The Knee Owner’s Manual.
6 Meniscus Tear Types That You Need To Know About:
1. Horizontal tear (Longitudinal)
This is an up and down or front to back a tear in the meniscus. Many times these tears are in a portion of the meniscus that does get blood supply (red zone) so could potentially heal on their own. Physical therapy is a first-line treatment that often works. If they do not heal naturally or with physical therapy, then arthroscopic surgical repair can sometimes be tried to help. A surgical meniscectomy should NOT be done for these types of tears as they can make the knee worse. PRP (platelet-rich plasma) or bone marrow concentrate (BMAC) containing stem cells can heal these tears as an alternative to surgery. These are more natural, safer, and have easier recovery than surgery so these should be done prior to considering surgery in most cases. They can also be used in conjunction with surgery to improve surgical results.
2. Radial tear (transverse)
This is a left-to-right tear across the meniscus. These are the most common types of tears. Most commonly they are in what we call the white zone of the meniscus where it does not get much blood supply. Thus, they are hard to heal naturally. PT should still be the first line treatment but these may benefit more from PRP or bone marrow concentrate (BMAC). If you see a surgeon, they will likely try to cut this part out (meniscectomy) despite the evidence saying that a meniscectomy does not work and can make the knee worse, so this rarely should be done for these types of tears.
3. Intrasubstance tear (incomplete)
Usually, these are degenerative tears in the midportion of the meniscus. After age 30, these are very common findings of a meniscal tear on MRI, which is of little consequence. Physical therapy is the first-line treatment. Typically, if you have pain, it will be from other knee issues such as arthritis. For mild to moderate arthritis, PRP has excellent evidence it can help. If the arthritis is more moderate to severe then BMAC will be a better treatment option. Most surgeons will not even try to operate on these as surgery doesn’t help and meniscectomy can make the knee worse.
4. Bucket-handle tear
This is a tear where the meniscus is torn and flipped over like a bucket handle. These sometimes can cause some catching or alter the motion of the knee. If that is the case then those would be the rare type of tear that actually would need surgery if that is the case. Typically, a meniscectomy is done as these may not respond to repair. If this type of tear doesn’t have the mechanical symptoms or knee catching/locking, then it possibly can be helped with physical therapy, PRP, or BMAC.
5. Flap tear
This is where a small piece of the meniscus can be torn and flipped over. Sometimes this can cause some catching of the knee, sometimes it does not hurt. If there is no catching in the knee, then it would not warrant any surgery to remove that part of the meniscus. Physical therapy would be a first-line treatment, with PRP or BMAC being an option. If it is causing some catching or altering motion of the knee that might be another rare case where surgery is indicated for partial meniscectomy as these are difficult to repair.
6. Complex tear
The last of the types of meniscus tears is the complex tear, where you have a combination of different tears where it can be torn in multiple areas of the knee. Oftentimes when the surgeon sees these, they would attempt a meniscectomy again because most of the time these are difficult for them to try to repair.
Tear locations
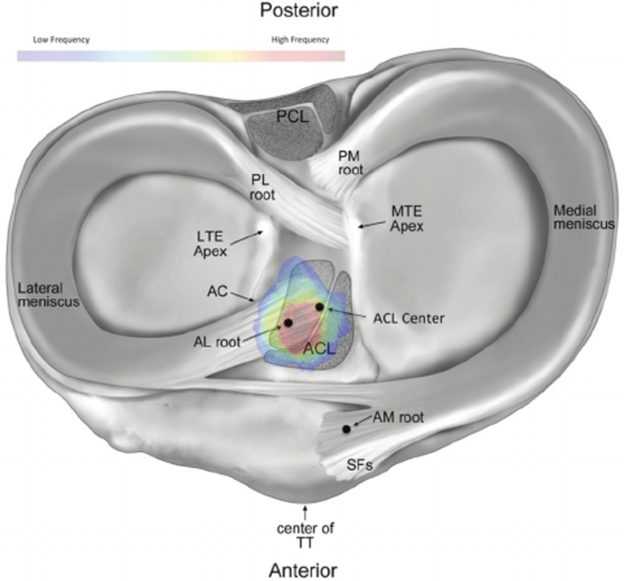
On MRI and or with some degree with ultrasound, you can determine where the meniscus is torn. This is important to know for treatment and to determine if the tear matches with a patient’s pain.
- Anterior horn: front part of the meniscus
- Body: mid portion of the meniscus
- Posterior horn: back part of the meniscus
- Root: front or back deeper part wear the meniscus attaches to the tibia
Risk Factors for a Torn Meniscus
The meniscus can be torn with sports, high-intensity exercise, trauma. Risks would be being overweight, low physical activity levels, or doing too high of intense exercise without being in proper shape, or having incorrect form/biomechanics. Typically, movements like knee twisting, deep knee bending, rotating the knee can predispose to injury.
Natural Remedies For a Torn Meniscus
If you have knee pain and have been told you have a suspected meniscal tear either from an exam or from MRI, much of the time, this can heal on its own with 4-6 weeks of rest, doing some physical therapy that would focus on some range of motion and strengthening exercises and correcting maybe any biomechanical problems that may stem from the core, back, hips or the ankles. Nutritional support such as just working on a healthy diet, reducing inflammation in the body, taking some turmeric, fish oil, glucosamine, and chondroitin, can help knee pain and inflammation as well.
Revolutionary Treatments For A Meniscal Tear Without Surgery
- If you go to most pain practices if you fail physical therapy and surgery is not yet recommended, they may recommend a steroid injection, which can help temporarily reduce inflammation in and around the knee and meniscus, but this is not advised as steroids as we know can cause damage to the joint cartilage, inhibit healing, and has a host of other negative side effects.
- An injection of something called hyaluronic acid, which is a part of some of the lubricating fluid of the knee joint could be used for temporary pain relief. It does not help repair the area but may provide a few months of symptomatic benefit if there is not severe arthritis in the knee.
- Meniscal surgery actually doesn’t have any evidence that it help meniscal tears and does have clear evidence that it can progress arthritis faster (2-8).
- If you actually want to try and get the body heal that meniscus on its own where rest and physical therapy did not do the job, PRP has excellent evidence that helps with meniscal injuries as well as mild to moderate arthritis that can be associated with these. PRP when used in the right hands, should be injected precisely with ultrasound guidance into the torn parts of the meniscus, into any ligaments or tendons that may be injured or loose and into the knee joint itself for optimal results. Many practitioners just inject into the knee, which still can help quite a bit but not as much than if a more thorough approach is taken. There are more than 25 high level studies showing PRP helps with knee pain (Orthopedic Bone Marrow Stem Cell Historical Timeline (netdna-ssl.com)).
- Bone marrow concentrate that contains stem cells within it can also be used for more severe meniscal tears or if there are meniscal tears with more moderate to severe arthritis. There are a few randomized control trials that show that this can be helpful for that as well (9-11). Again, you want to have a thorough skilled approach to make sure that image guidance is used, and all of the damage parts of the meniscus and associated areas of the knee such as tendons, ligaments, and joints are injected as well.
The latter two options are what we focus on at the Centeno-Schultz Clinic, promoting the body’s natural ability to heal itself with PRP and bone marrow concentrate has been shown to be very successful, has little risk, maintains the natural anatomy and structure of the joint, and has more evidence that is positive compared to meniscal surgeries, which evidence shows that we pretty much should not do the surgery except for the rare cases of types of meniscus tears with mechanical symptoms, such as flap or bucket-handle tears.
Keeping Your Meniscus Healthy
Knee your knee and meniscus healthy but eat healthily (see Nutrition 2.0), consider supplements such as glucosamine and chondroitin that can be good for arthritis or our stem cell support supplement), reduce excess inflammation by eating healthy, keeping a normal weight, exercising, and maybe taking a supplement such as turmeric. Keep the knee strong with some daily physical activity like elliptical, biking, walking, and some resistance/strength training 2x/week. For exercise make sure you warm up before and cool down after, have good technique, and stay within your functional limits. Physical therapists, Egoscue therapy, foundations training, muscle activation therapy (MAT), trainers, and other types of body therapists can help with form, posture, biomechanics, and treat minor problems to reduce the risk of injury.
Bottom Line
Meniscal tears are common findings in the knee, which many times are of little clinical significance. What matters is the type of meniscus tear.
If a tear is associated with pain, depending on the tear, most of these can be handled with nonsurgical treatment measures. When the traditional measures of rest, physical therapy, diet, and supplements fail, then PRP and bone marrow concentrate for more severe problems can be a great alternative to promote your body’s natural ability to heal, reducing pain, keeping the natural anatomy, and reducing the risk for future surgeries. Meniscal surgery, despite being the most common orthopedic surgery has little evidence to support it and actually good evidence to suggest that we should eliminate the majority of these types of surgeries. If you or anyone you know has a meniscal tear or knee pain and is interested to see if you are a candidate for treatment, please contact us. We are experts at boosting your body’s natural healing ability through precise image guided regenerative interventional orthopedic procedures.
References
(1) Risberg MA. Degenerative meniscus tears should be looked upon as wrinkles with age—and should be treated accordingly. British Journal of Sports Medicine 2014;48:741. http://dx.doi.org/10.1136/bjsports-2014-093568
(2) Katz JN, Brophy RH, Chaisson CE, et al. Surgery versus physical therapy for a meniscal tear and osteoarthritis [published correction appears in N Engl J Med. 2013 Aug 15;369(7):683]. N Engl J Med. 2013;368(18):1675–1684. doi:10.1056/NEJMoa1301408
(3) Sihvonen R, Paavola M, Malmivaara A, Itälä A, Joukainen A, Nurmi H, Kalske J, Järvinen TL; Finnish Degenerative Meniscal Lesion Study (FIDELITY) Group. Arthroscopic partial meniscectomy versus sham surgery for a degenerative meniscal tear. N Engl J Med. 2013 Dec 26;369(26):2515-24. doi: 10.1056/NEJMoa1305189.
(4) Sihvonen R, Englund M, Turkiewicz A, Järvinen TL; Finnish Degenerative Meniscal Lesion Study Group. Mechanical Symptoms and Arthroscopic Partial Meniscectomy in Patients With Degenerative Meniscus Tear: A Secondary Analysis of a Randomized Trial. Ann Intern Med. 2016 Apr 5;164(7):449-55. doi: 10.7326/M15-0899.
(5) Netravali NA, Giori NJ, Andriacchi TP. Partial medial meniscectomy and rotational differences at the knee during walking. J Biomech. 2010 Nov 16;43(15):2948-53. doi: 10.1016/j.jbiomech.2010.07.013.
(6) Cohen SB, Short CP, O’Hagan T, Wu HT, Morrison WB, Zoga AC. The effect of meniscal tears on cartilage loss of the knee: findings on serial MRIs. Phys Sportsmed. 2012 Sep;40(3):66-76. doi: 10.3810/psm.2012.09.1983.
(7) Longo UG, Ciuffreda M, Candela V, Rizzello G, D’Andrea V, Mannering N, Berton A, Salvatore G, Denaro V. Knee Osteoarthritis after Arthroscopic Partial Meniscectomy: Prevalence and Progression of Radiographic Changes after 5 to 12 Years Compared with Contralateral Knee. J Knee Surg. 2019 May;32(5):407-413. doi: 10.1055/s-0038-1646926.
(8) Katz JN, Shrestha S, Losina E, Jones MH, Marx RG, Mandl LA, Levy BA, MacFarlane LA, Spindler KP, Silva GS; MeTeOR Investigators, Collins JE. Five-year outcome of operative and non-operative management of meniscal tear in persons greater than 45 years old. Arthritis Rheumatol. 2019 Aug 20. doi: 10.1002/art.41082.
(9) Centeno C, Sheinkop M, Dodson E, Stemper I, Williams C, Hyzy M, Ichim T, Freeman M. A specific protocol of autologous bone marrow concentrate and platelet products versus exercise therapy for symptomatic knee osteoarthritis: a randomized controlled trial with 2 year follow-up. J Transl Med. 2018 Dec 13;16(1):355. doi: 10.1186/s12967-018-1736-8. PMID: 30545387; PMCID: PMC6293635.
(10) Hernigou P, Bouthors C, Bastard C, Flouzat Lachaniette CH, Rouard H, Dubory A. Subchondral bone or intra-articular injection of bone marrow concentrate mesenchymal stem cells in bilateral knee osteoarthritis: what better postpone knee arthroplasty at fifteen years? A randomized study. Int Orthop. 2020 Jul 2. doi: 10.1007/s00264-020-04687-7. Epub ahead of print. PMID: 32617651.
(11) Hernigou P, Delambre J, Quiennec S, Poignard A. Human bone marrow mesenchymal stem cell injection in subchondral lesions of knee osteoarthritis: a prospective randomized study versus contralateral arthroplasty at a mean fifteen year follow-up. Int Orthop. 2020 Apr 23. doi: 10.1007/s00264-020-04571-4. Epub ahead of print. PMID: 32322943.