I want to be careful to separate the physician from the procedure; I will state early on that the problem is not surgeons but their lack of having a safe and effective tool for HEALING the meniscus. Blogs in the next few days will discuss the currently available treatments with stem cell therapies for regeneration of the meniscus.
Now, on to the evidence…..
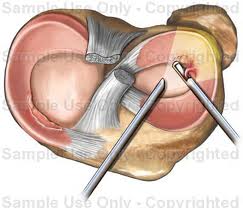
A recent MRI study of meniscus tears showed that radiologists weren’t very good at determining which tears were best suited for arthroscopic trimming or repair (http://uk.reuters.com/article/idUKTRE6BT3EF20101230). Data doesn’t generally support that surgery is a good idea for most meniscus tears in the first place (see below), so a study that looks at how good or poor MRI is in telling surgeons if they will have to trim the meniscus or suture it, makes little sense.
In addition, another study showed that meniscus tears are equally common in middle aged patients with knee pain and those without knee pain. This begs the question whether in most middle aged patients, a meniscus tear is even relevant as something that causes pain, let alone whether we should be operating on these tears. Now add in studies showing that cutting out pieces of the meniscus only leads to the onset of knee arthritis (http://www.ncbi.nlm.nih.gov/pubmed/18751768).
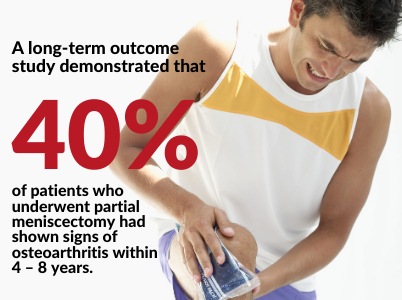
How about another research study showing that when these knees with meniscus tears and stretched or torn ligaments are operated with arthroscopy, they still get arthritis the same as when they’re not operated (http://radiology.rsna.org/content/early/2010/05/31/radiol.10090683.abstract)? Here’s one that showed that treating a degenerative meniscus tear with arthroscopic knee surgery fared no better than just leaving the tear alone (http://www.ncbi.nlm.nih.gov/pubmed/17216272)? How about this one (just published), showing that partial menisectomy (the arthoscopic trimming of the meniscus discussed above) results in changes in knee biomechanics that lead to more joint contact and that this likely explains the faster onset of arthritis in knees that have had this surgery (http://www.ncbi.nlm.nih.gov/pubmed/20719317).
In summary, surgery for meniscus tears, while common practice, isn’t supported by the totality of the published research.